THE CALL
I got the call at 3 am February 8, 2024. I answered the ringing iphone, snatching it off the bedside charger. Phone calls at 3 am are almost never good. This one was THE CALL.
Two women from the transplant team at Beth Israel Deaconess were on the phone. One was a cardiologist, the other a nurse practitioner who we had already met and really liked. They told me that a match for me had been found and they were offering me a heart. I wasn’t prepared for that term “offer”. Being half asleep it confused me.
I managed to ask a few questions. The only thing they could disclose was that the donor had been declared brain dead. It is explained to the patient once they are on the wait list that when this call comes in, the patient needs to decide then and there. If for some reason the patient declines, the system needs to move to the next person who is a match on the wait list. Time is critical.
I said “yes”. I was instructed to pack some things and come to the Klarman Building at Beth Israel Deaconess. My wife Lauren and I loaded a gym bag and headed into Boston. It was a little eerie driving through the cold dark deserted city streets at 4 am. We parked in the usual lot a block away and walked to the front entrance.
KLARMAN BUILDING – Beth Isreal Deaconess Medical Center – Boston, MA

An area that was usually a beehive of activity was void of any light or people. The front glass entrance was dark. The large, automated double door opened and in the unlit lobby an imposing security guard asked us if he could help. I said, “Well, um, yes. I’m here for the heart transplant”. He told us to follow him.
It was spooky walking those halls. It was like the large quiet modern building was mildly sedated. We got in and found the place where we needed to be and got settled in a room. That day is fuzzy to me now. I have patches of memory that tell me part of what happened. My wife Lauren remembers more. I was not wheeled into surgery until 8 pm so we were there more than 14 hours.
I recall signing forms. All the usual questions. Current medications were reviewed. When I last ate. Vitals taken. I stepped on a big metal scale for my weight. I was NPO (that stands for Nil Per Os: which in Latin means Nothing By Mouth). These past years Lauren and I had come to call that NOPE. Meaning, “NOPE, can’t have anything”. We were old hands at NOPE at this point.
Each of my three daughters came over during that day and sat with me until I was taken to surgery. One of my daughters asked if I was nervous or afraid. I honestly replied that I wasn’t really. Maybe a little. Like the apprehensive feeling one might have in the dentist chair prior to getting a crown. I can’t say for certain why I wasn’t terrified. I think it was partly my faith and that I trusted I was in God’s hands regardless of the outcome. I had lived on the edge of the abyss for so long at that point. I was very confident in all the people we had met at the medical center. And what choice did I have? I was ready for whatever came next.
During this wait time I was washed head to toe in a roomy shower with special soap twice. At some point, once on the table under warm towels they shaved me where they needed to shave.
While on the wait list I did have kind support from one friend who was a heart transplant recipient. During my 3 years on the wait list, we had talked several times on the phone and met for breakfast. Over several conversations he had been very reassuring. In essence he described it as a hard recovery and some life changes that need to be adopted post-transplant. He had managed it well for 5 years.
My Dad had said something to me as a kid once. I was nervous about something, swimming lessons maybe. He said “Listen kiddo, when you are there, look at the boy on your left. Then look at the boy on your right. If they can do it, then you can do it.” Then he snapped his newspaper and went back to reading.
They brought me into the prep area at 8pm. Then the memory completely fades out. My wife and daughters went across the street to a hotel that generously provides a discount for patient families. I was told later the operation started at 9 pm and ran until 3 am the next morning February 9th. Then I went on ECMO.
THE TRANSPLANT
Several separate surgical procedures were required for me during this operation.
First, the heart transplant itself. I think most people reading this understand that this kind of operation requires a sternotomy. A vertical incision is made from the top of the breastbone (sternum) to the bottom where the ribs join. The chest is opened with a sternum saw to gain access to the heart so that the diseased heart can be surgically removed, and the donor heart can be inserted in its place. During the operation I was put on a cardiopulmonary bypass machine that pumps and oxygenates the blood.
After the operation, the chest is closed, the sternum is rejoined using titanium wires and the skin is stitched closed. The nine inches of stitching is covered in medical glue. After the surgery while in recovery I got curious and I googled up what a sternum saw looks like. There are many types; however, they all look like a high-end model of a cordless tool made by DeWalt or Milwaukee that you might buy at Home Depot.
THE CRTD
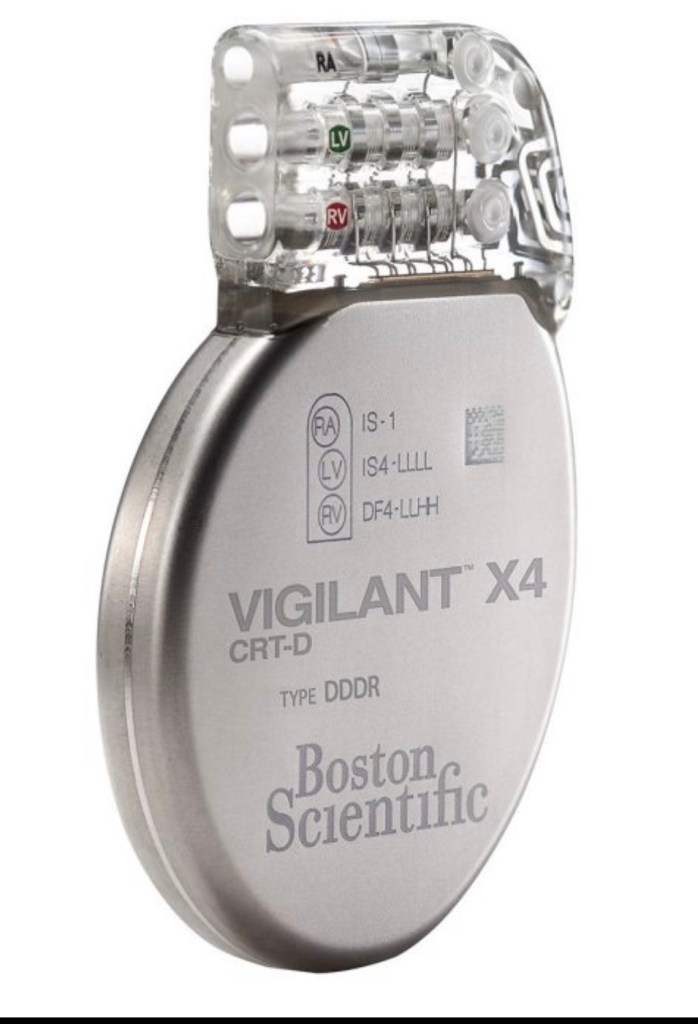
The second procedure was the removal of my implanted CRTD. CRTD is an acronym that stands for Cardiac Resynchronization Therapy Defibrillator. This device had been attentively keeping my heart pacing and me alive for over 3 years.
It served three functions. First, as a pacemaker. It was pacing me at about 96%, which means my heart was providing 4% of the pacing.
It also serves as a defibrillator in the event my heart should fall into a dangerous arrhythmia. For me that was a sustained Vtach. Were that to happen, it delivers a jolt or shock of energy (41 joules) if the heart rate climbs above or below preset parameters. This shock brings the heart back out of the arrhythmia and back to sinus rhythm. My parameters were set at 220 beats per minute on the upper end.
Lastly, the resynchronization function provides the heart assistance with the atrium and ventricle chambers being in sync and the timing of their opening and closing working together. This makes the ailing heart as efficient as possible. Later, I will have a separate post that cover aspects of this device.
I was getting a new heart, so I no longer needed the CRTD. It resided on my upper left chest just below my clavicle and it’s about the size of an old-style stopwatch that would fit in the palm of a hand. 3 wires, called leads, snaked from the CRTD thorough my blood vessels and into my heart where they were securely affixed with tiny threaded screws. The CRTD, and the leads all came out along with my damaged heart. They made an incision to remove it right below the old incision that was made 3 years prior to implant it.
CHEST TUBES
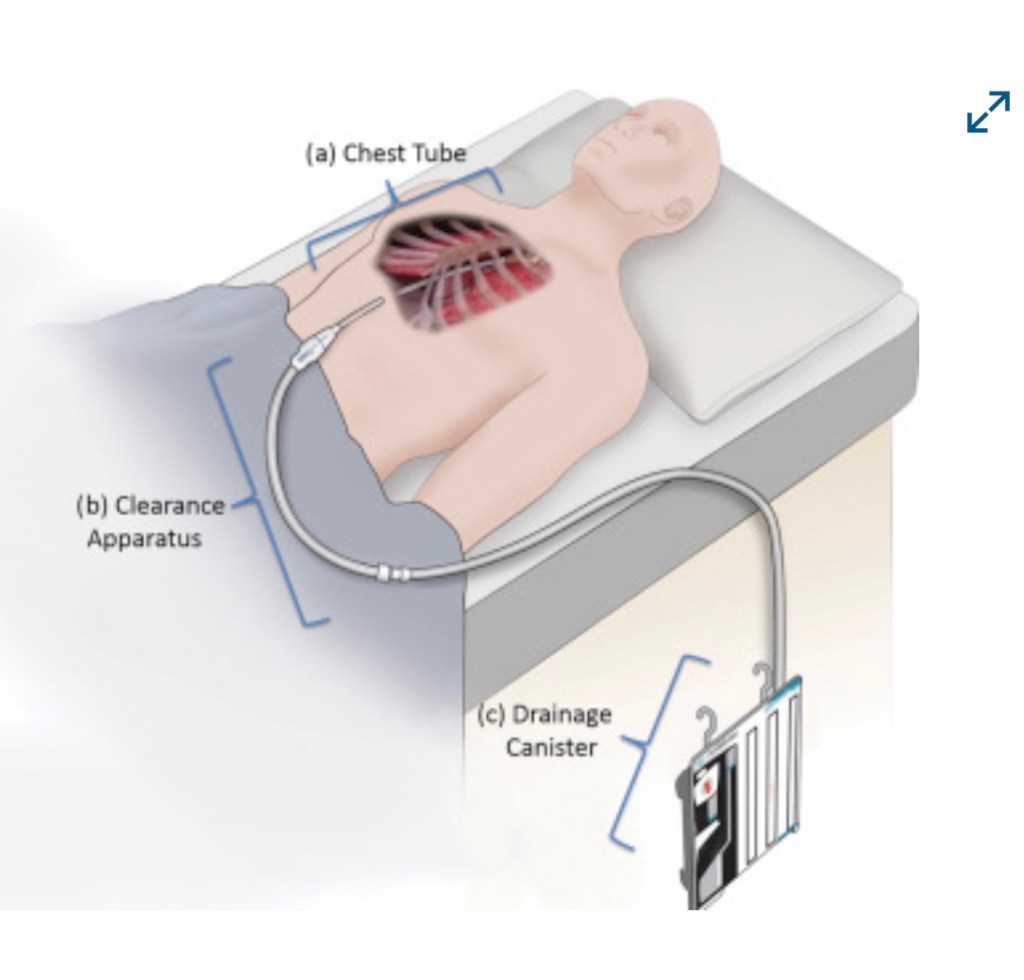
Another procedure that rides along with getting a heart transplant is having chest tubes that are surgically placed just below the bottom of the sternum incision. There are two holes placed to accommodate the hoses which lead to drainage canisters that rest on the floor beside the bed. These chest tubes are there to drain away air, fluid and blood that could otherwise end up in the chest cavity and cause problems.
These chest tubes are removed a few days after the surgery in recovery.
ECMO
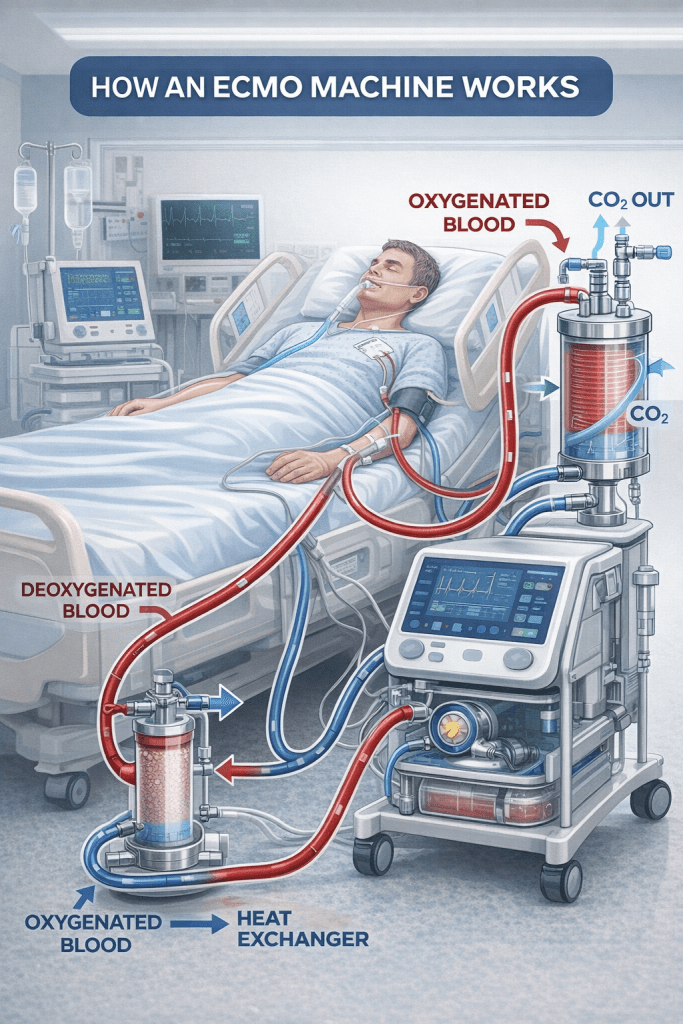
The third procedure they had completed after the transplant itself while I was under anesthesia was to put me on ECMO, or Extracorporeal Membrane Oxygenation. An ECMO machine essentially does the work of the heart and lungs if the new transplanted heart needs a little help getting started. Sometimes the heart is a little stunned coming from one environment to the other. Who can blame it? ECMO is needed in about 5-10% of heart transplant cases.
For ECMO, the transplant team needed to make a large hole in my groin and another in the upper right side of my chest. These incisions are there to accommodate tubes that carried my circulating blood supply. For visualization purposes of these tubes, think small garden hose.
I was also intubated.
So, all that said, there is a lot going on there. A brilliant soft-spoken Japanese surgeon who did this operation is the Surgical Director of Heart Transplant at Beth Israel. He had amazingly done over 300 heart transplants in the NY area prior to moving to Boston. Heart transplant was new at Beth Israel and he was a big part of its beginning. I am heart transplant number 14. He met with Lauren afterwards and said, “The operation went fine, he is on ECMO”. A man of few words.
The operation went from 9 pm February 8th to 3 am on the 9th and I was on ECMO for 2 and half days until the morning of Sunday February 11th.
Clearly this summary is a brief oversimplified review of what took place. It is a description that is within my capability. My goal in this series of essays is not to explore the miraculous granular detail of what went on but rather give a sense to others of the general operation I had. Of course, I was not aware of any of it. You go under anesthesia in one room, wake up later someplace else.
I have been and continue to be astounded by the skill and dedication of the surgeons and supporting specialties who do this work. The fact that there are people who can do this is as beyond my comprehension as a thing can be. Deep appreciation toward everyone on the medical team, I have found, is universal to all heart transplant patients I have met.
I had some strange dreams and visions at some point as I began to emerge from 4 days of anesthetic unconsciousness . I will try my best to describe as best I can it in the next post.

Leave a comment