
By Phil Liaboe
The metaphor I adopted and used from the start was borrowed from the Wizard of Oz. I was determined to Follow the Yellow Brick Road. Just like in the old movie, this is not a straight path. It is filled with twists and turns. If they tell me to turn left, I will turn left. Scary stuff jumps out of nowhere when you least expect it, as you will see if you continue reading these posts. But I figured if I do my best to follow the instructions I am given from the transplant team, and with help from Lauren, then I will have the best result that I can have, long term.
After the initial shock wears off a regular routine settles in. The medical staff is highly attentive. They are testing and monitoring progress to make sure everything is on track. They are also educating, because the patient and caregiver will be doing much of this at home very shortly.
There is a daily rhythm that settles in and little by little I started to feel stronger. Some advice to anyone facing this, measure your progress in weeks, not days. I did not make great progress day to day. I made tremendous progress week to week.
One by one the twelve or so monitors and pumps that were next to my bed after the operation were removed. I was still only vaguely aware of this. Lauren would say, “Oh look, you are down to only 4 now.” Eventually there were none.
What was challenging for me was keeping up with the information being delivered. Starting with the introductions. Doctors enter the room and immediately introduce their names and titles. Cardiology, Electrophysiology, Pharmacy, Dietician, Diabetes, etc. This gets rattled off quickly. We learned to ask them to please repeat the introductions. We just wanted try to slow the pace down. It feels like everybody is moving in hyper speed. I felt like I was in wet sand.
CARE TEAM
Here is a breakdown of people helping make this a success.
Nurses:
At Beth Israel Deaconess, every day in the initial recovery floor there are 2 nurses that change shifts every 12 hours. Each 12 hour shift has a Registered Nurse (RN) and Certified Nursing Assistant (CNA) doing various tasks related to patient care. I was determined to learn, pronounce and record each of their names and find some way to send a thank you afterward. Sadly, I discovered over time that a thank you later was just not possible for a variety of reasons. I did try to converse and get to know these folks, call them by name and express my appreciation as much as I could.
CNAs were usually students from the many higher education institutions the area. The CNA does many of the routine checks and vitals that are needed all day and all night. Blood glucose level, weight, blood pressure, temperature, are all checked many times throughout the day and night.
RNs administer the meds and have overall responsibly for general patient care and communication with the transplant team. They were all, to a person, outstanding! No exceptions. One thing that was solidified in my mind was how underpaid these people are. Several times I heard from some of them that they were here only in Boston temporarily and that they could not stay in the area because it was too expensive.
Doctors and other medical staff come in the room all day long for a variety of reasons. It is helpful to know their titles and what they mean. What authority or level of training they have is indicated to an extent by their title. None of this was clear to me during my stay. Here is a very basic summary what they are:
- Medical Students: Learners completing clinical rotations.
- Interns: First year of residency after medical school
- Residents: Physicians in specialty training (e.g., internal medicine, surgery)
- Fellows: Physicians who have completed residency and are training in a subspecialty
- Attending Physicians: Fully licensed, board-certified (or board-eligible) physicians. Ultimate responsibility for patient care and clinical decisions
HEART MONITOR
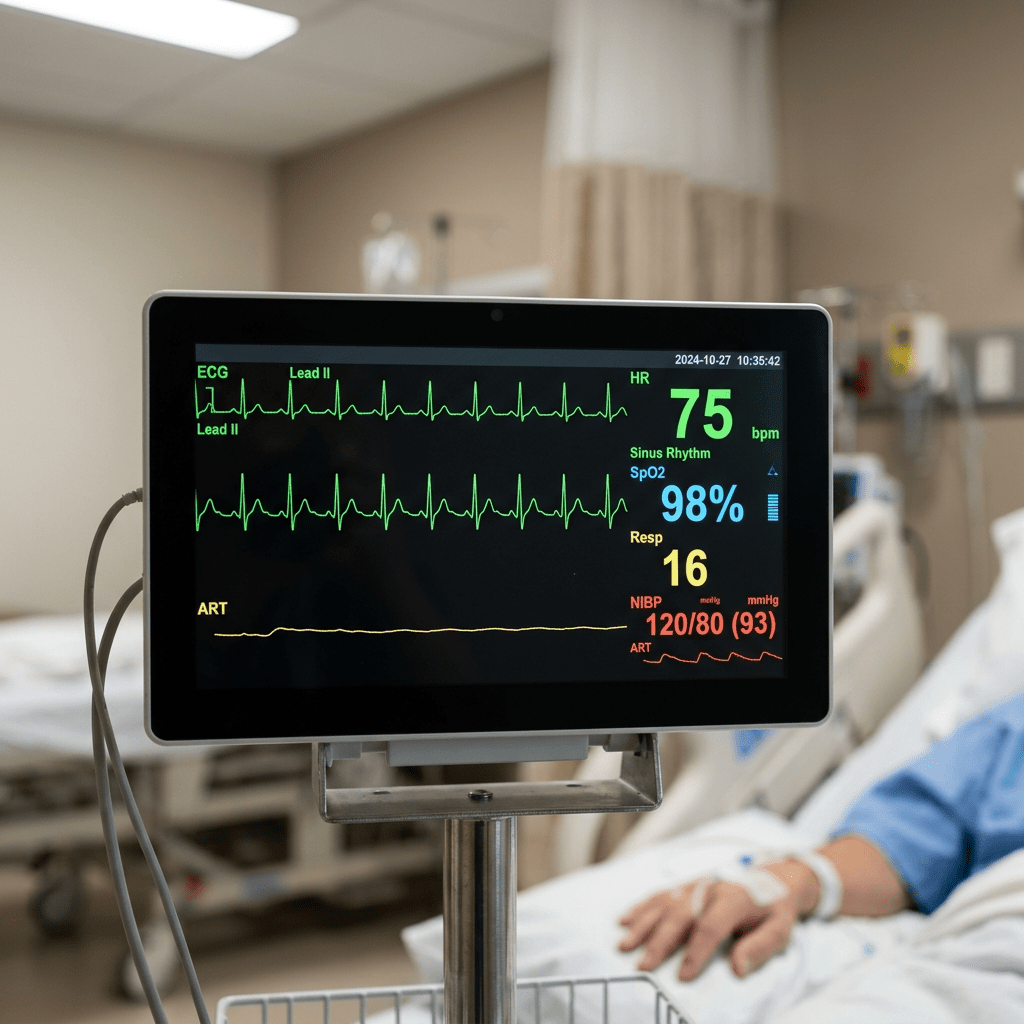
The entire time in the medical center until discharge I wore a heart monitor. Adhesive leads are placed at various locations around my torso. Wires from leads run to a small telemetry device about the size of small cell phone. This device transmits a continuous real time data feed of my heart activity. This data is displayed on a monitor in my room, on a display in the hallway outside my room and at nurse station outside my ICU room door. I loved looking at my perfect sinus rhythm line on the display. Prior to transplant, it looked nothing like that.
PICC Line

Every day blood is drawn and checked several times. The good news is that the blood is drawn through a PICC line. PICC stands for Peripherally Inserted Central Catheter. The PICC line gets placed early in the admission process with ultra sound guidance and stays there until discharge. This eliminates needle sticks for blood draws. It also facilitates other medical purposes like IV meds etc.
CHEST X RAYS
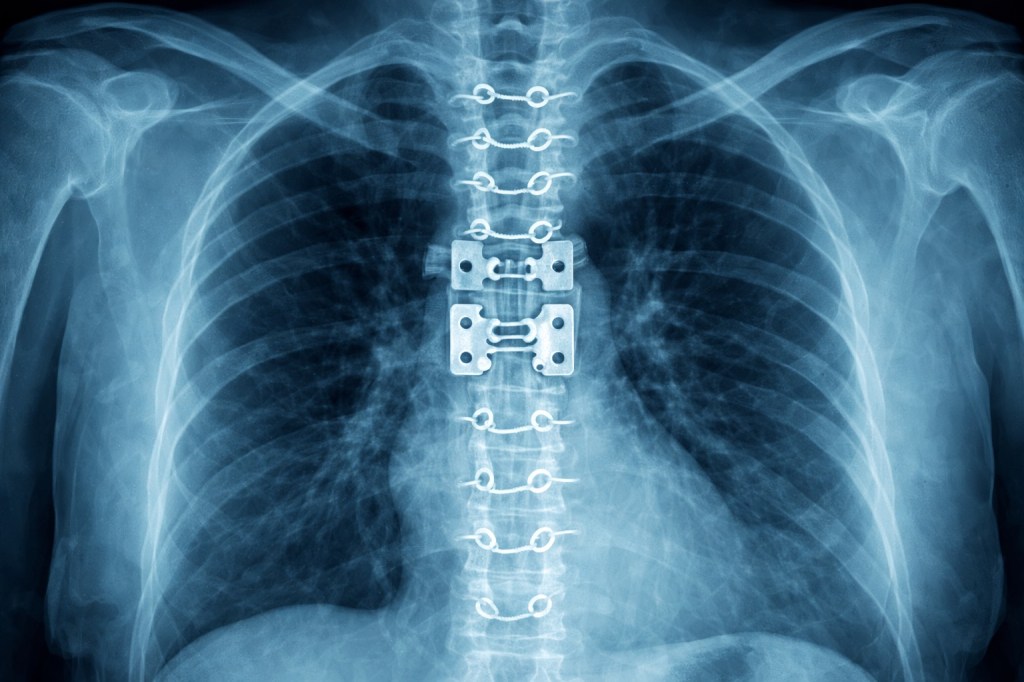
I remember getting chest x-rays. I would get these every day it seemed, but in this case the chest x-ray came to me. A technician wheels the x-ray machine into the room. A metal casing about one foot square, called the image receptor, was nestled between my back and my inclined bed. Then a heavy flexible lead shield was draped across my lap. The machine was lined up for the best position and the x-ray was taken.
FLUIDS
Getting the fluid out means taking a diuretic. Mine was BUMEX or Bumetanide. This was another new experience for me. The first time I took a BUMEX I filled up almost two 1000 ml urinals in an hour. Also, the staff is measuring everything being consumed, eating and drinking. They are also measuring everything going out, urine and bowel movements. Later when I could walk to the bathroom there is a device just under the toilet seat that catches everything for measurement.
TIP: When taking BUMEX, once you get that first little signal that you need to pee, begin the process to get your urinal ready immediately. You don’t have much time.
To assure that pneumonia does not set in, I was given a device where I was to inhale to raise the disc to higher and higher levels. I was to use this a certain number of inhales per hour. This became easier from day to day and later brought it home where I continued to use it.

BLOOD GLUCOSE
Blood glucose is checked constantly. At least 5 or 6 times a day it seemed. 2 things cause blood glucose to rise are:
- The body’s reaction to significant physical trauma causes a massive release of sugar into the system.
- High doses of steroidal medications like prednisone increase glucose levels.
I became temporarily diabetic. Slowly it trailed off and after 2 years I no longer take any meds for blood sugar. This does not happen to everyone. I needed occasional insulin injections during my stay. This continued after discharge. I will go into this later with the discussion of medication management needed once the patient is home.
ROUNDS
The Attending doctor usually accompanied by a Fellow will stop and visit and do a thorough exam. Check the heart and lungs with a stethoscope. Get patient input. Check the incisions. One unusual part of this exam is the doctor will press a closed fist slowly but deeply into the lower abdomen. This caused zero pain. While doing this I was asked to turn my head so they can see indicators in my neck for fluid.
The doctor is getting an estimate for jugular venous pressure. Some numbers are recorded and over time I learned that 6-8 cm was normal. A reading of 8–10 cm suggests fluid overload. Ankles are also checked for swelling. That is a good indication of fluid presence.
SLEEP, OR LACK THEREOF

Sleep for me was tough. I hated the hospital bed. I mean it was a fine bed, but I hated it. The room had a reclining chair, and I would try to sleep in that to no avail. I even tried to curl up on the mini sofa also in the room. One night a nurse came in and was alarmed because the bed and chair were empty and all she saw was a guy lying awkwardly on the sofa.
I have discovered over time that anesthesia and prednisone really mess with my ability to sleep. I have dealt with this by accepting it. I don’t fight it anymore. I’ve tried everything. I have been on a steady diet of prednisone for over 6 years. I will sleep when I can sleep. I might not feel great while I am awake, but shit happens. It’s just the way I roll I guess.
I could not read, which is my “go to” at home when I can’t sleep. Reading was just a level of brainwork that was not operational quite yet. I tried to watch a movie on my iPad and could not get it to work. A few days later I discovered that the reason was I had not connected it to the hospital WiFi. An important step that I had completely lost in the fog.
The hard part about not sleeping is that during the day there is a lot going on. Nurses are educating me about meds. Various doctors of all kinds are stopping by to check on important topics. Family members and friends are calling. I got through it ok and all but at the time I was always just kind of a zombie. Not unlike when our kids were babies and I had to work after not sleeping for successive nights, over a period of months.
Doctors that would stop by and ask how I’m feeling and I would tell them I am not sleeping. Then they would brush past that answer and ask “well ok, tell me how your heart is feeling…”. Sleep was not high on their list of concerns, which I get. They provided some Ambien but it had zero effect. In fact, it seemed like once I took the Ambien, I was even more awake. Eyes like big old fashioned light bulbs wide open all night. A nurse would quietly sneak into my dark ICU room in the middle of the night to get some blood from me, or quietly check a monitor or something, thinking I was sleeping and I would say “HI”. They would jump, startled. Then ask me why I was awake that I should be sleeping. I know.
MY NEW PASTIME
As the days went on and I made progress walking the precautions regarding falling dropped away one by one. First, I overcame the need to have a backup nurse behind me. I held tight to an empty wheelchair by the handles in back. Then I was approved to walk the corridor without holding on to a walker or the back of a wheelchair. They told me to walk as much as possible. I loved hearing that.
The hallway had markings on it representing different milestones on the Boston Marathon. From Hopkinton to the finish line and a half dozen or so landmarks in between like Heartbreak Hill and Boston College. These markings are on the corridor wall down toward the floorboard. Each session the goal was to get a little further along the route. In a few days I was doing the entire hallway. I then graduated to multiple laps.
I had a new hobby at night when I could not sleep. I emerged from my room clutching my heart shaped pillow to my chest at 3 am and would walk up and down the hallway eventually crossing in front of the nurses desk. They would always say the same thing. “You should be sleeping”. I know.
At the end of the hallway was a large double door operated by waving a hand in front of it to get out and enter the lobby and elevator area for that floor. Keep in mind that this building, the Klarman Building, was newly constructed. The lobby and elevator area on each floor was a very clean and spacious area with floor to ceiling windows at least fifteen feet high looking down on Dana Farber Cancer Center and across the city of Boston. Each floor’s lobby had a uniquely themed artwork. If I lived nearby, I would be tempted to just go there and read or or hangout even if I wasn’t sick.
So after walking the hall and being in my room for days on end I was feeling stronger and wanted to go out there in that nice lobby and sit. I waved at the blue sensor and shuffled out there through the double doors. I had my red pillow tight against my chest while I was talking on the phone to a friend. I facetimed him to show him how great the place was. I was out there about five minutes when a nurse poked her head around the corner and asked me nicely what I thought I was doing.
She told me I was not allowed past the double doors. Furthermore, the mobile heart monitor telemetry device I had on did not work while I was out in the lobby. The nurses saw a “no signal” at their station and began looking for me. She said that if they cannot find a heart transplant patient it’s not a good look. They ushered me back to my room and told me I should be sleeping. I know.
After a week I was moved from the ICU to a different floor. A floor for patients no longer needing intensive care. It’s called the “Step Down Telemetry Unit”. It was very evident right when I settled into the new room that the level of supervision was dramatically reduced. Lauren and were feeling like, “Hey, where is everybody?” This feeling of being “cut loose” continues at every step of this process. Of course it’s a good thing. It’s a strange feeling.
DENERVATED HEART
During the walking and later when I was cleared to climb some stairs, the denervated aspect of the heart became apparent.
Denervated is pronounced {den er vated}, but the word is derived from the principle that the heart has been {de nerve ated}.
When a heart transplant occurs, nerves that control communication from your heart to the brain are severed. Specifically, the vagus nerve and the sympathetic cardiac nerves. This is permanent. This results in the following:
- Higher resting heart rate: For me, as I am typing this my resting heart rate is 94. That’s my new normal. This is not from lack of physical activity. I get some form of fairly rigorous exercise 5 or 6 days a week.
- Slower response to exercise start: The heart rate rises more gradually. Example: Climbing a flight of stairs or a hill, I don’t feel the need for more breath until I am at the top or later. This is a little weird at first.
- Slower response to exercise end: Even though I stopped exercise, an accelerated heart rate continues longer. I noticed this right away too. When I get my heart rate up to 130 BPM for example, it’s takes a long time once my exercise has stopped before it’s back under 100.
After reading up a bit on this the simplest way I can understand this is that post-transplant the brain gets signals through hormones in the bloodstream instead directly from nerves. That new process is slower and takes more time for the heart to react.
NURSE STORIES
One of the nurses taking care of me had just lost her cat. And when I say lost, I mean it was gone. Her husband was in the military stationed somewhere out west and had been re-assigned to a post near Boston. During his drive east with all their belongings, outside of El Paso, the cat had jumped out of the truck through an open window. This nurse said that now her cat was living it’s best life chasing mice out on the plains of West Texas.
I had one nurse who gave us an excellent recipe for potato leek soup. Lauren made it one of the first days I got home. It was amazing. This same nurse had a toddler at home, and her husband was on a business trip in Banff. Banff is a big ski resort town in Alberta, Canada. He had a conference there that lasted 5 days and he was extending it to 8 days because he liked to ski. This nurse is on a 12-hour shift with a baby at home and her husband EXTENDS his “business” conference in Banff? The next day I saw and her she said her husband had returned but he was exhausted and went right to sleep for about 14 hours.
Then there was nurse Wu. There is a song by the band Steely Dan called “Dr. Wu” from the Katy Lied album. It’s a great song musically and lyrically. Spotify it up and check it out. The lyrics fit my situation perfectly. From then on that song was my newest theme song. I started calling her Dr Wu.
One of the nurses had a name I for some reason recognized as being from Nepal. We chatted about how long she had lived here and how she liked it. I asked her if she had lived in Katmandu and she said she did. I asked her if she had been to Mt Everest and she said no. Really? I was amazed. It’s only 100 miles from Katmandu to Mt. Everest. Don’t they have some picnic tables or something at the bottom? I asked her if she had ever heard the Bob Seger song “Katmandu”. She had never heard of it. Later that week she saw me and said she had listened to it, loved it, and sent it to all her friends back home.
And there were many others. One who rode motorcycles. Another one who sat with me while we compared the Catholic and Lutheran faith theologies. She went to parochial catholic schools prevalent in the Boston Area from K though 16. She wanted to know the differences. Finally something I know!
I discussed their experience with the Covid pandemic. It was a horrifying and it made me feel very bad that this one particular sector of people got slammed so hard by this event. It caused some to quit their livelihood. Imagine working 24 hours shifts taking care of dying COVID patients and then going home to your family. Some family members being elderly, or cancer patients or other vulnerable people. Having some patients curse you because you required them to wear a mask. Our society asks a lot from people who don’t earn very much relative to the contribution.
Without exception, the nurses and doctors who cared for me were real angels. Men and women with a calling. I truly felt that they loved their calling and the job they had and that love spilled over to me.
I am close to discharge! With that in mind I will write about managing medications which is paramount an once we are home, it is all up to us.
© 2026 Phil Liaboe. All rights reserved.

Leave a comment