By Phil Liaboe
12 Times over 18 months – After Transplant
This is an invasive procedure that for the heart transplant patient serves several purposes. First it measures pressures, fluids and various heart functions. It also facilitates taking small samples of heart tissue post-transplant to be tested for signs of organ rejection. Any rejection activity needs to be treated ASAP to prevent damage to the organ. After my heart transplant the schedule for this procedure was as follows:
- Once per week for the first 4 weeks.
- Once every other week for the following month.
- Once per month for the next 3 months.
- Once every other month until the first-year anniversary.
- After the 1st anniversary, as needed. I will explain.
One key result from the test is whether the patient is experiencing any organ rejection from the transplanted heart, sometimes referred to as the “graft”. The test results are reported in this scale:
0 = No rejection
1R = Mild rejection, but not enough to require treatment
2R = Moderate Rejection – Treatment required
3R = Severe Rejection – Aggressive treatment required
THE FIRST ONE
I had my choice of whether or not I wanted to be sedated. I only used sedation for this first one, which was just a few days after the heart transplant operation. I was wheeled into the operating room in my hospital bed. I was unable to walk. The team there asked me if there was any chance I could maneuver over from my bed to the table. I said “Yes – 2 chances. Slim and none.” The space between the two tables, about 3 inches, looked like the Grand Canyon.
Recall I had been told to not use my hands or arms to move around in bed due to the fresh chest incision in the early healing stages. The operating room attendants said, “no problem”. They deftly maneuvered my body to slip something underneath me. A button was pressed somewhere and what can only be described as a small tight inflatable life raft suddenly surrounded my body. With a gentle push I was seemingly floated from my bed to the procedure table. I never knew such a device existed. Look it up on YouTube. Air Assisted Transfer Mattress. It’s pretty cool. The mattress was deflated once I was on their table. I was hooked up to the sedative they asked me to start counting backward from 100. I woke up back in my room. All done.
SUBSEQUENT PROCEDURES (#2 – 12+)
For the rest of my scheduled RHC / Heart Biopsy procedures I elected no sedation. This is not unusual. The real advantage to having no sedation is that I was allowed leave the recovery area after only a few minutes. Those with sedation need to hang around in recovery for an hour or longer. Plus, without sedation I was avoiding that snowed under feeling the rest of the day. I told that to a nurse once. She said “Ya know, some people relish that snowed under feeling for a day”. Point taken.
PREP
I know this process now like the back of my hand. I have had 12 of these in the last year or so. Again, this is not intended to be an accurate medical accounting of what this procedure is, but rather a description of what this was like for me. My best recollection. I did not interview any doctors or nurses.
After a review of the risks, medications I am taking and some consent paperwork I am escorted into the clean, sterile and technology packed catheterization lab. I remove my shirt and hang it on a hook and don a johnnie. For the most recent ones I didn’t even remove my shoes. I lay down on a table and they begin the prep.
It’s always cold in the room and they always offer me a heavy warm blanket. For the first couple of these I felt so lucky to have a warm blanket. Wow, I thought, this must have just come out of the dryer! Great timing! Turns out these blankets are stored in a warming enclosure. I never said I was very bright. Leads are stuck on my torso for the heart monitor. I can hear the beeps of the heart monitor and see the sinus rhythm on the display.
Sometimes the work is done by a Fellow. A Fellow is a doctor who is in advanced specialty training. In that case a cardiologist is supervising. Other times the work is done by one of the cardiologists.
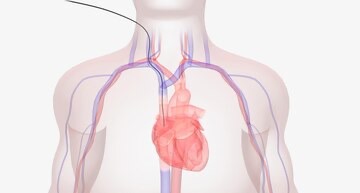
I turn my head as far to the left as I comfortably can exposing the right side of my neck as much as possible. I’m told not to move my head from this position until it’s done. Various coverings are draped around my body and over my head leaving a patch of exposed skin on my neck where they will be working. The coverings are positioned so the face and mouth are not covered. My request. I’ve learned that if my face is covered it gets stuffy and I feel a little claustrophobic so I ask that my face not be covered.
Since my head is turned so far to the left, I cannot see anything or anyone on my right side, where the work on me is happening. An imaging device is lowered from the ceiling to hover directly over the working area, my chest, and controlled by a rail system in the ceiling. The image from this device is projected onto a very large monitor to assist the doctor in guiding the instruments.
A LITTLE STING
Shortly thereafter I hear the words from the doctor “something wet and something cold here” while they clean the patch of skin on my neck with anti-bacterial solution. Translation, “Nothing sharp yet”. Then a bit of jelly is applied so that an ultrasound wand can identify the best entry point in the jugular vein. Still nothing sharp. Then come the magic words, “OK – now you’re going to feel a sting and a burn”. Something sharp.
This is numbing medicine, not the actual catheter insertion. That is the only uncomfortable part of the procedure for me. One of those contrarian moments in life. The only pain is from the injection of the numbing agent. How much pain is somewhat dependent on the physician doing the injection. It’s not bad. A sting and a burn.
MEASURING PRESSURES AND FLUID
Once all that is done, they get to work. A catheter is inserted. The only thing I feel is pushing and pulling on my neck. I will say the first few times I was a bit surprised at how much pushing and pulling is involved and the amount of force that is being used. I can feel and have awareness of them stuffing instruments down the tube in my neck and pulling them back out. Apparently, it takes some force.
The catheter is a narrow tube where instruments will be inserted and withdrawn several times. Since my head is cocked left and the doctor is working on my right side, I am able to watch the large monitor on my left, along with the doctor as the work is being done.
The first instrument that is inserted into the catheter through my neck down into the heart is a Swan-Ganz catheter. The name Swan-Ganz comes from the inventors who figured out that if you put a tiny expandable “sail” on the end of this instrument, the blood flow will use the sail and carry it to the different chambers of the heart in the blood current.
Jeremy Swan was a cardiologists on the west coast of the U.S. and an avid sailor. He had been having difficulty getting catheters to travel where he needed them in the heart. Observing sail boats and the behaviors of spinnakers he decided to use the same principle on a catheter where blood would be the guide. A small inflatable “sail” at the tip brings this instrument to the desired chambers of the heart. This is inserted, pressures and fluids tested, then removed. I assume both Swan and Ganz get a few bucks every time one of these disposable little instruments gets unwrapped.
I can hear the doctors calling out numbers. I assume these are my pressure and fluid readings. Who exactly is recording these figures is not clear. At the far end of the cath lab is windowed room with people in it.
HEART BIOPSY
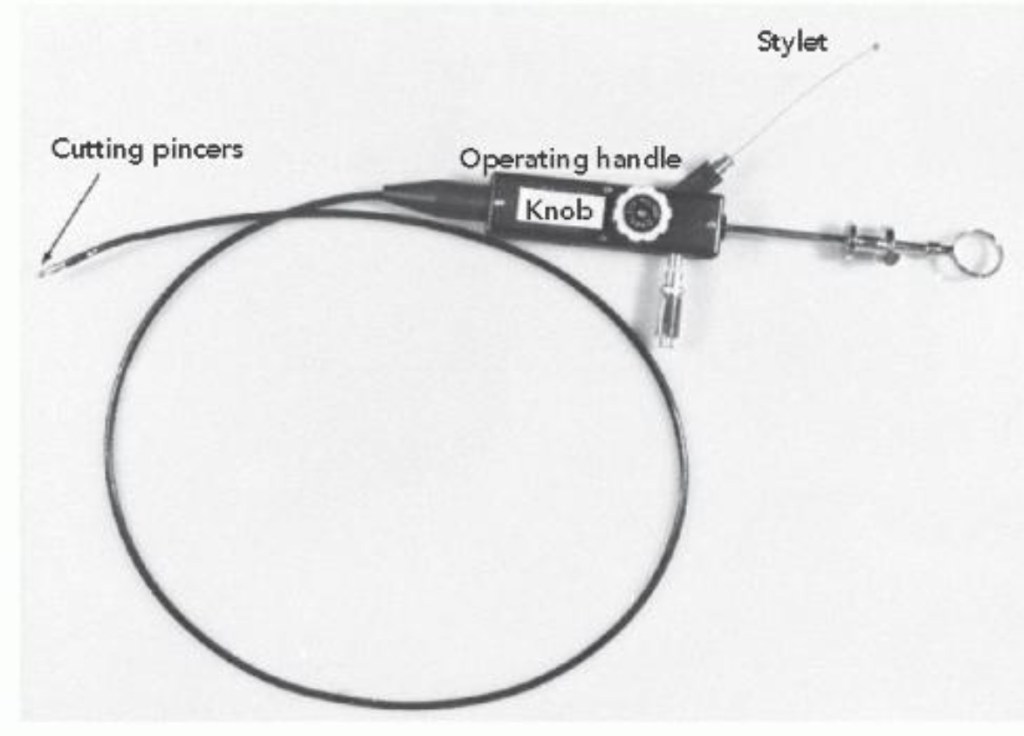
Another instrument used is one that will extract samples of heart tissue and is called a bioptome. This small flexible tool has forceps at the tip for clipping off tissue for sample testing. A half dozen samples are taken. Sometimes more. The samples are very small. The reason they need to take so many is that some of the samples will not be useful for the biopsy test. For example, some samples may have too much fat content. The doctor does not know this at the time of extraction. For each sample, this tool is inserted, the tissue is clipped off, then the tool is extracted. In and out, several times, which explains all the pushing and pulling. I can also hear a whirring noise, like a fishing reel being cast. This is the instrument rubbing against the catheter during insertion and removal.
One might wonder if this damages the heart. I did. I was told it does not. There are areas in the heart where these samples can be taken without bringing harm to the organ.
Watching all of this on the monitor fully awake gets kind of boring. Although I am watching the monitor, as a patient with zero training, I can’t really interpret what I am seeing. It’s about 45 minutes total. On most of these procedures at some point I fall asleep. We have to leave the house very early for these. We had to sleep fast the previous night. I haven’t had any coffee because I’ve been NOPE (nothing by mouth). One thing I do feel is those old familiar PVC sensations while they are rummaging inside my heart. I can’t say I enjoy feeling that.
There is usually very soft murmuring and whispering between the Fellow and the supervising Cardiologist. Sometimes I can make out a phrase or a word. They are communicating between themselves but for some reason don’t want me to hear. I have picked up little pieces like “a little more to the left”, or “no, higher – yeah, that’s good” or “yeah that one looks good”. Hushed guidance and exchanges.
On some of these, when they have inserted the catheter at the beginning I will feel a stream of liquid flow down the side of my neck. They are opening the jugular so I assume it’s blood. The Fellow quickly dabs at it with gauze and says “Oops – sorry!”. The Fellow is not apologizing to me. He or she is apologizing to the supervising Cardiologist. Halfway through they usually ask, “Hey there Phil, are you doing OK?”. I tell them that I am, and to let me know if they need some help.
That’s it. Done. I get a big bandage on my neck that looks like I was grazed by a stray bullet in a hunting accident. I am given instructions for the next 24 hours. No shower. No lifting. I get a sheet of paper with instructions if something goes amiss. Nothing ever never has. Since I had no sedation, I hop down off the table and get dressed. I thank everyone who helped me as they clean up the room and start to prepare for the next patient. I walk out to the waiting room to my smiling and patient wife, ready to drive me home or to the nearest restaurant since I’ve been NOPE since the previous night.
WAITING FOR REJECTION RESULTS
Then I wait for the notification on my phone that pings me telling me I have new test results. The doctor tells me right away after the procedure how my fluid levels and pressures look and he if doesn’t I know now to ask. The test results that contain information related to rejection take a day to two to get back. This is usually a period of mild anxiety for me.
All of my rejection scores have been either 0 or 1R, except once. I did get a 2R and that earned me a 3 day admission for IV infusions to fight the rejection. This happened due to an unusual complication specific to my case, which I will get into later.
After a half dozen of these heart biopsies a bit of scarring starts to show on the lower right part of the neck where the instruments enter. It becomes something you recognize in other heart transplant patients. Sort of like a tattoo, except that nobody would know what it means except other people who have been around heart transplants. The scarring looks like a very small patch where there may have been some stubborn acne in the person’s younger years. It appears toward the side of the neck so collars mostly cover it. Over time it largely disappears.
CARE DX
In lieu of the RHC / Heart Biopsy, another method the transplant team uses to check for rejection is a special kind of blood test. This is ordered periodically to keep close tabs on rejection in between heart biopsies. The two tests conducted by this blood draw are AlloMap and AlloShore and each will yield a score (delivered to your portal) that measures risk of rejection in different ways. The score will show the patient if they are in the green, yellow or red. Clearly these blood tests for organ rejection involve less risk to the patient than a heart biopsy.
Allomap – This score gives an indication if the body’s immune system is gearing up to reject the heart.
Alloshore –This score indicates if the transplanted heart is being damaged by rejection.
For me, this blood draw is managed by a company called CareDX. It is drawn at my home (not a lab) and driven directly to the medical center where it receives special immediate handling to the testing location. The results from this blood draw use a different scale than the heart biopsy.
Indications of rejection on this test generally then results in a RHC / Heart Biopsy to confirm the status and severity. This test also creates for me a bit of mild anxiety awaiting the results.
PERSONAL NOTE
Nobody wants to be someone who needs to be “taken care of”. I never thought I would be in this position. For each of these procedures so many important tasks need to take place without fail. The prep call, the nurse staff, the physicians, and of course my lovely wife of 36 years. I feel very grateful that all the skill, care and kindness afforded to me along this path. At times it is overwhelming.
The next post will describe the removal of the chest tubes.
© 2026 Phil Liaboe. All rights reserved.

Leave a comment