By Phil Liaboe
Managing Meds – Part 2
I realize this is not the most exciting topic. It deserves 2 separate posts because of it’s importance. At discharge the pharmacy in our medical center delivered a big paper sack to my room containing all the medications we needed to get started along with a jumbo pill box. They included a blood pressure cuff, a digital thermometer, and a high quality scale for my weight tracking.The nurse practitioner spread all the pill bottles and other items on the bed and instructed us to fill up the pill box. They wanted to make sure we knew exactly what to do prior to leaving.
I was still dazed and confused so this final test fell mostly to Lauren, who was amazing. She was checking the 3-ring binder they gave us against the other written instructions they had provided, and she was finding discrepancies and pointing out typos to the staff. I was watching her work, wanting to get home and crawl under a comforter on my sofa. I was so grateful she was “on point” and organizing it all for me. I could not have done it and at the same time I could not have stayed there one more night. I wanted to get home so bad I could taste it.
THE PILL BOX
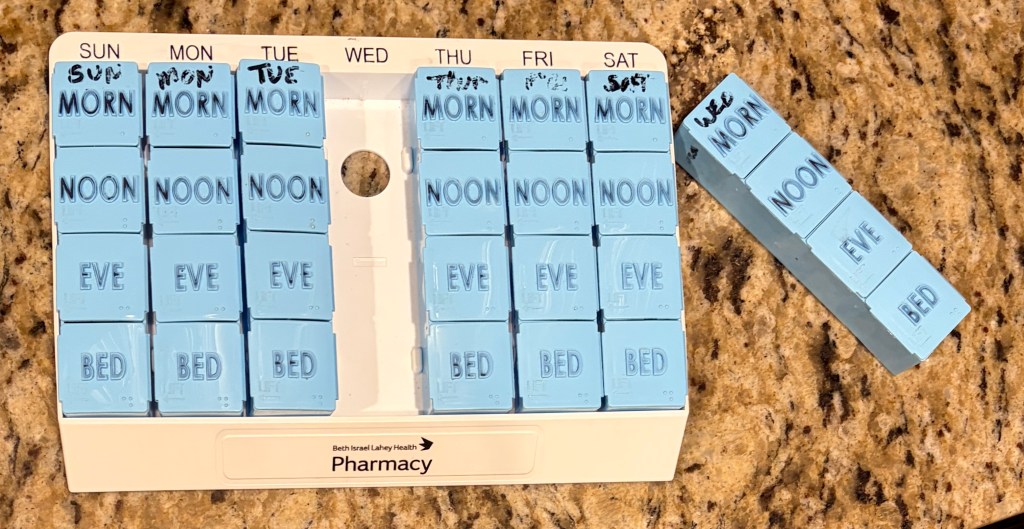
The pill box is a larger version of anything I had seen previously. Every day of the week has a separate removable column and every column has separate compartments for morning, noon, evening, & bedtime. If I know I am going to be out of the house during a time slot when I need to take meds, I bring that column with me. If I don’t want to take the whole day’s meds with me, I transfer the meds I need while I’ll be gone to a separate single pill box. We keep a one-day supply of my meds in each car in case I forget to bring them, or if I was delayed wherever I was and did not get home in time to take the next batch.
In addition to filling the pill box, we needed to learn how and when to inject insulin. After my transplant I was temporarily diabetic. I had never been diabetic before. We needed to learn how to check my blood sugar and what readings would require an insulin injection. The insulin injection pen is pictured above. The blood sugar result dictated the amount of insulin to inject. This is a multi-step process which I will not describe in detail here. The sequence of steps were not easy for me to grasp when I was 10 or 11 days post-transplant. Plus a needle is involved. Watching it for the first time with the shape I was in I could hardly follow along. A few weeks later I was doing it like breaking sticks.
All this information may seem overwhelming at first. It was to me and to us. Lauren dove in and understood everything quickly. I came around gradually. I still struggle with aspects of this after almost 2 years. We try to use all of tools we can think of to help us. We keep a well-organized spreadsheet as was described in the previous post.
COSTS
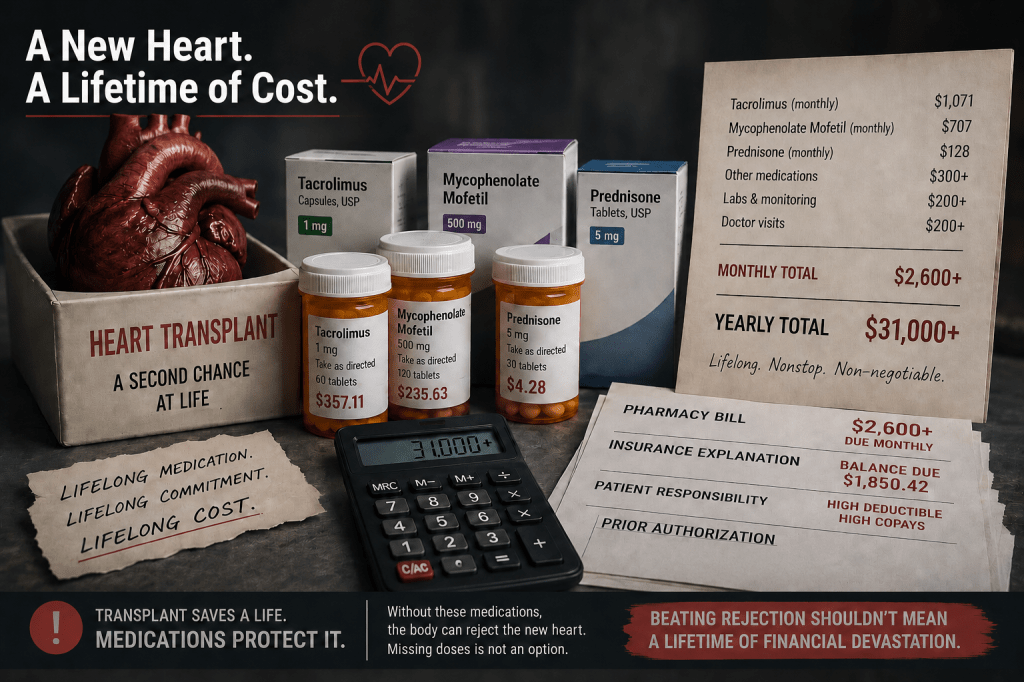
I am going to avoid any advice on where to buy medications. Everyone has a different situation and there are many options. If in doubt and we have a problem of some kind, we ask our transplant coordinator for guidance. They have faced these challenges before, and we are doing this for the first time. Our transplant team has used avenues or provided ideas to minimize costs, particularly on those items that are expensive.
I am on medicare so I am allowed, under the policy, to acquire some medications under Part B instead of Part D in medicare. I am also pleased to report that some meds that are on the expensive side have assistance programs through the drug manufacturer. As an example, Farxiga is made by Astra Zeneca. Farxiga was a medication I took when I was in advanced heart failure. Astra Zeneca has a program to assist people who qualify with discounted or free Farxiga. I qualified for assistance and Astra Zeneca delivered my meds to my home free like clockwork. A highly efficient and responsive organization.
Lauren bought a cheap plastic pill splitter. It helps us save costs. A word of caution, not all pills are meant to be split. We check first. Some pills have a coating that is important and is defeated if the pill is split. Pills that are OK to split are “scored” to make it easier. The dose changes can be managed sometimes by splitting pills which can save some money.
When the transplant team has told us that I can stop taking a certain drug, we don’t dispose of it. We keep them all until expiration because I might need to resume taking it. Same applies if the dose changes. We keep everything until it expires.
THERAPUETIC RANGE
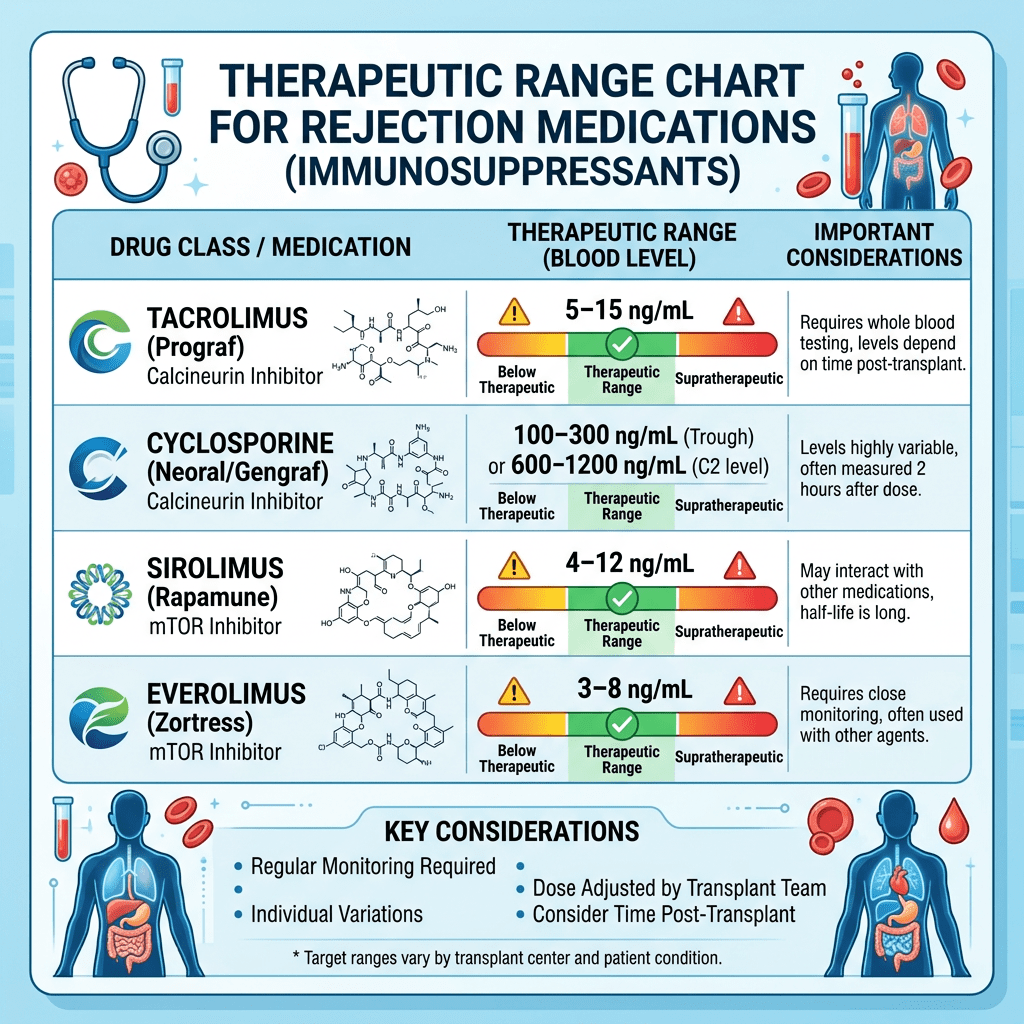
One of the aspects to anti-rejection meds is that this type of medication needs to stay within a therapeutic range. As an example, my therapeutic range for combined tracrolimis and sirolimus is a blood test result of 8 to 12. This is determined by a blood test for this specific medication. Blood is tested frequently for me. My case is a bit unusual for reasons I will detail later. Currently I take 1 mg of sirolimus in the morning. I take .5 mg of tacrolimus in the morning and 1 mg at night. I had a blood draw yesterday and today I got the result of 4.7 for sirolimus and 4.1 for tracrolimus so the combined score is 8.8. I am in the theraputic range. No change this week and I will retest in 2 weeks.
TIMING
Timing some of this blood test is very important. The blood test for the anti-rejection drugs needs to be done 30 minutes either side of when I take that medicine AND must be prior to that day’s dose. So, in this case I take sirolimus at 9 am every day. To test for that med to see if I am in the target range, I need to have the test done between 8:30 am and 9:30 am before I take it that day. It is preferable to be as close to 9 am as possible. Finding a lab that I was comfortable with was key. Not too long of a wait. Not too many people in the waiting room. It is very helpful if the lab reports the results directly to the transplant team and the Primary Care Physician (PCP) and to my portal at Beth Israel. For most of my 2 years post transplant I have had blood drawn for this purpose almost weekly. It is just beginning to become less frequent.
It deserves mention that we try to keep a healthy, if not abundant supply of all the meds we need. We try to ask for 90 days for every prescription we are allowed to. We are not dooms-dayers; however, we do try to keep as much on hand as we can in case of unforeseen future supply chain disruptions. We strive to avoid running out by accident.
We buy as much as we can over the counter. Some examples are calcium supplements, baby aspirin, and magnesium.
BALANCING ACT
Recall I wrote that this whole endeavor is like a science project? The overall goal for heart transplant patients and these medications as it has been explained to me is to seek a balance between preventing rejection and preventing infection. These are conflicting goals.
Anti-rejection drugs lower the body’s immune system to a point where the organ is not rejected by the natural immune system. Doing this naturally leaves the body more susceptible to unwanted infections of all kinds. The body’s ability to fight off common bacteria, virus and fungus is reduced. Cuts on the skin, certain foods, sun exposure (skin cancer) and even a common cold are to be treated with extra caution.
Treating the management and execution of the instructions by the medical center cavalierly and routinely missing doses poses two risks. Risk number one is rejection of the precious donated heart. I don’t think I need to go into why that is bad except to say that even a little rejection can cause some heart damage that is irreversible. Risk two is that the patient gets a serious infection. A spiked fever, pneumonia, infected cut or a wide range of other physical problems could land a patient in the hospital.
My wife and I went on a very nice cruise to Alaska about 18 months post-transplant. The medical center had cleared the trip but said to be careful. We were. I came home with a wopper chest cold and bad juicy cough that my doctor diagnosed as pneumonia. I took prescribed anti-biotics for a few days and avoided serious illness. I was not clear of this nasty bug for 2 months. And that was with not missing any doses.
IT GETS BETTER
The good news is that over time, the number of medications for me has been reduced. For example, I became less diabetic and now take no diabetic meds at all. Other meds are reduced in dosage. As I said earlier, some are lifetime and the management of those meds by the transplant team will go on for a long time, I hope! Blood draws become less frequent but never go away. Routine tests for rejection via blood draw will continue and provide the team my real time status.
When my transplant first happened, I viewed all of this as a nuisance. Something I had to do but did not think about too much except when an alarm went off or when the pill box needed refilling.
Now my attitude has raised this activity from a nuisance to a primary and important part of my day. This was caused by me missing doses and being determined to not do that. And, sometimes I still do, but much less often. I acknowledge that these pills are keeping me alive. I am thankful that God put on this earth people and organizations that created this technology that keeps me alive. Mostly I’ve come to the gracious recognition that this is all my responsibility.
I am also not going to delve into the topic of big pharma and all the aspects of how meds are developed and how they are priced. This is a very complex subject and includes wide array of topics involving the FDA, Higher Education research, public funding and companies that are striving to make a profit. If you are interested in this topic, I can recommend a book I read recently called “Rethinking Medications” by Dr. Jerry Avorn. This book was recommended to me by a close friend and it was very interesting. I think it would be interesting to anyone even if they were not dealing with lots of meds. While the system we have today appears on many levels to be corrupt and broken I do feel grateful that the system has these meds for me right now.
I think it is totally within anyone’s purview to question any medication being prescribed. We look them all up on ChatGPT. We ask what alternatives there are. We ask what the side effects are. We want to show the medical team that we are engaged and active in decisions regarding my health. While I cannot say enough about the level of care we have received, we acknowledge that we are not the only patient they have. On the other hand, my wife and I right now have only one patient, me. We watch things very closly and we (really Lauren) have caught the occasional minor slip-up by our medical team. Nobody is perfect. 3 sets of eyes need to be on this. The patient, the caregiver and the medical team.
The next post will be about being discharged and going home. Many times being discharged from the hospital means you are good to go. You’re done. As a heart transplant patient it means it has only just begun.
© 2026 Phil Liaboe. All rights reserved.

Leave a comment