
Cardiac Rehabilitation
By Phil Liaboe
I was skeptical when it was explained to me that two or three months after my heart transplant I would be prescribed by the transplant team to attend eighteen weeks of cardiac rehabilitation. Twice a week! I was not convinced that there was really anything I could learn. I felt I knew a lot about exercise and thought it was going to be like other physical therapy experiences I’d had over the years for sports related injuries.
Whenever I had been through physical therapy in the past it was always the same. I would start attending and quickly learn the exercises I needed to do. I could do them at home. I would attend three or four sessions and take the offered sheet showing which exercises I should do and then I was done. I had the discipline to carry on, on my own. I was a believer. I just didn’t think in this case it was really important to attend something twice a week for over four months. It struck me as overkill.
FOLLOW THE YELLOW BRICK ROAD
In keeping with my commitment to follow the yellow brick road I followed the program to the letter. Out of the thirty-six prescribed sessions I missed only one session and that was due to a heart biopsy that was on the calendar that could not be moved.
I learned a lot. It helped me a great deal. In fact, it was amazing. All my previous assumptions were wrong. I came out of that program feeling better, stronger, more confident and more knowledgeable than I ever could have dreamed. I came in a little wobbly. I left with a bounce in my step that surprised me in a very positive way.
Once I was cleared by the medical team to start it proved difficult to find a cardiac rehabilitation facility that could fit me in. Not for any other reason than supply and demand. We all understand that heart disease effects a tremendous number of people in America and cardiac rehab is prescribed for people who have had all sorts of heart problems and operations. People who are recovering from heart attacks, by-pass surgery, valve replacements, and whole wide range of other patients are prescribed to go through this kind of program. I was the only heart transplant patient I saw in my program during the 18 weeks I attended.
LOWELL GENERAL HOSPITAL
After some persistence I was able to get into the facility of my choice which was Lowell General Hospital. It is within ten minutes of my home. It took about a month of frequent calls and follow-up. A technique my wife refers to as “badgering”. In the basement floor of this hospital, with small windows that touch the ceiling looking out at ground level, is a rehab area that as you might expect resembled a small gym. There were twenty or so different types of cardio machines including treadmills, ellipticals, rowers, and stationary bikes.
In the middle of the room against one wall was a long table containing the workspaces for the medical staff which consisted of a mix of four or five nurses and physical therapists and their laptops and other gear. This crew of medical supervisors stayed the same over the course of the twice a week, eighteen-week program. Only cardiac rehabilitation patients use this facility.
A class consisted of ten to twelve patients. The ratio of patient to medical supervisor was usually about 3 to 1. I had signed up for the eleven o’clock time slot. Each patient in a class is at a different point in their rehab program. The day I started, I walked into a class of people who were currently at any point of the beginning, middle or toward the end of their program. My first day was a bit like when I was the new kid when our family moved from St. Louis to Minneapolis when I was in the 5th grade. Everyone at school knew what to do and where to go except me.
Every patient attending every session regardless of how far along they have progressed follows the same specific routine once the class starts. At eleven o’clock the receptionist who checked us in and gave us each our white identifying hospital wrist bands announces to all of us that the previous class is done and we are free to enter.
Upon entering, patients go through a multi-step process.
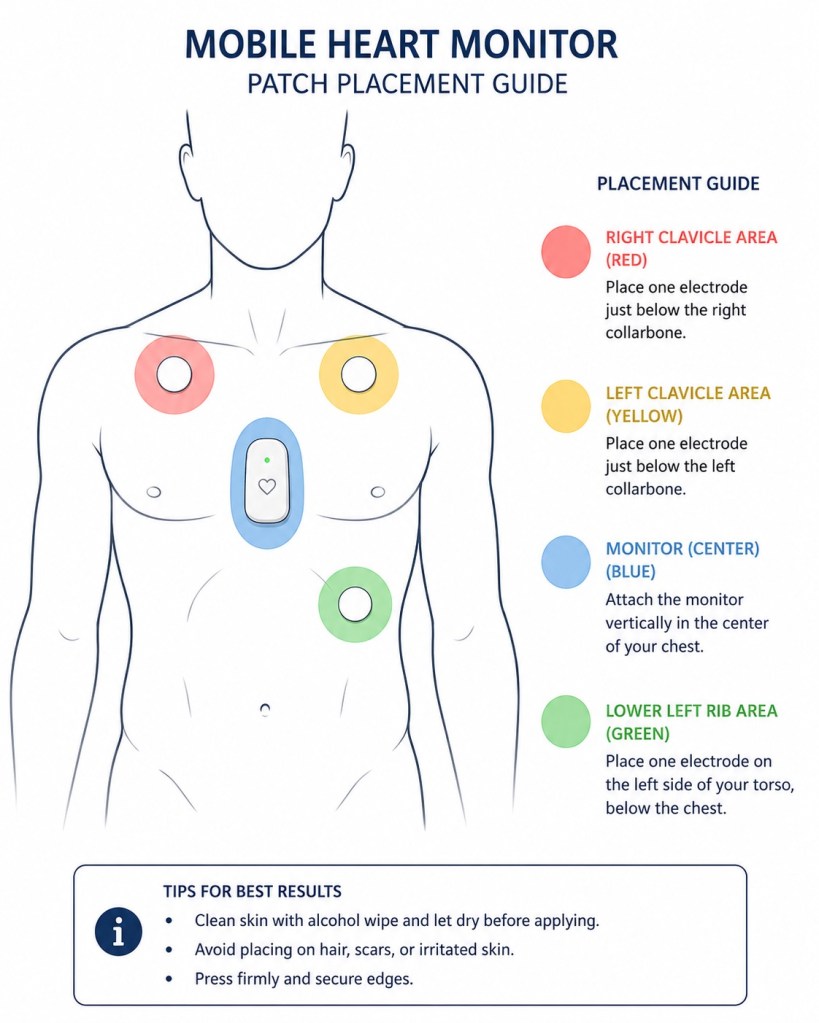
STEP 1 : The patient attaches a mobile heart monitor to their own torso. These monitors are in a pile and are numbered. Each monitor has several wires, each with color coded sensors and adhesive to attach to the skin under the shirt. A chart on the wall shows the outline of a human torso to provide guidance for the appropriate locations for the patient to attach each color coded sensor. The monitor itself is placed in a soft pouch hung around the patient’s neck.
STEP 2: Once the monitor is attached, each person proceeds to the central main table and takes a seat. The medical staff takes and records the blood pressure, temperature, heart rate and in some cases blood sugar of each patient. In my case they never tested my blood sugar.
STEP 3: The patient hands the medical staff a slip of paper that has data to be entered into the system. It includes the monitor number the patient just attached, and answers to some basic questions like: Are you feeling well today? Any changes to your medications? Etc.
While one nurse is taking the vitals, another is entering the data including the patient’s monitor number. Given that the monitor number identifier is entered into system now each person’s heart activity is shown by name on several monitors high up on the wall. At a glance, the medical staff can see how any individual is doing from a heart activity perspective at any time during the session from anywhere in the room.
STEP 4: The last step prior to beginning rehab activity is for a nurse to provide that day’s list of exercises that was prepared by the staff in advance. Approximately forty-five minutes of movement including warming up, working out and stretching.
EXERCISES
I clearly recall while I was going through my exercises the first day thinking that it was really easy. Too easy. Or so I thought. The warm-up was just walking on a level treadmill for five or ten minutes, then seven or eight minutes on three different cardio machines, and then six stretch moves, each held to a count of ten.
On the cardio machines, there are settings to increase or decrease the level of difficulty. These settings are determined by the medical staff. A nurse swings by after the patient has been using the machine for a couple of minutes and asks two of three basic questions such as:
On a scale of one to ten how difficult is this right now?
Are you short of breath?
How are you feeling?
The staff is getting a sense for how fast to bring the patient up to the next level of difficulty. At least once during the workout portion of the class the patient’s blood pressure is taken a second time. After stretching patients go through the same process they did checking-in only in reverse. I would grab a chair near the medical staff command center and they would take my blood pressure for the third time, temperature and heart rate and I would turn in my custom workout slip. Once the heart monitor is removed the session is over. The room is empty for fifteen minutes while the medical staff buttons up from the class exiting and prepares for the class coming in.
That first day I kept telling the staff the exercise was too easy. If I was going to be there I might as well get the most from this. An old lesson from my Dad was that if you have no choice and you are required to be somewhere or do something (like school or work) then do your best. Pretty simple advice. That is what I was determined to do.
It was easy to see that if someone wanted to sail through going easy it would be fairly simple to just tell the nurses that the machines were set too difficult. Patients quickly learn that the responses given to questions asked about difficulty and breathing are used to determine the next sessions custom workout. The idea, of course, is to gradually increase the level of exertion if not each session, certainly each week. But this was done very slowly. Nearly imperceptibly. I came home after that first day, thinking during the session it was a breeze, and I was a wet noodle the rest of the day. I was toast.
Early on I was assigned to be supervised by one of the more experienced nurses. A very bright energetic woman who gave me the impression she knew some of the unique physical limitations I needed to deal with. I asked her a question one day after having been in the program for a few weeks. I wanted to know if I could take my grandsons hiking on a popular climbing trail called Mount Monadnock located in southern New Hampshire. She quickly did some research which entailed converting the hike into METs or Metabolic Equivalent Tasks. She checked the distance, the altitude, my weight and concluded that, yes, it would be no problem. I could handle it.
As time went on, I gradually felt less and less like a wet noodle. As the sessions progressed week after week, familiarity set in. Normal banter and conversion between patients and the medical staff became less awkward for me as we got to know each other. We learned about each other’s families. I watched people graduate and the whole class cheer. I watched while others started, their first day, stumbling through the process as I had, trying to attach their heart monitor wondering what to do and where to go.
One of the most enduring memories of my time there was the noticeable level of care and attention that I had from the second I entered the room, until I left. I began one of my sessions, having received some very bad news the previous day. That day was very difficult for me. My emotions were at my throat, and it took enormous effort to tamp them down. Very early on during that workout session one of the nurses, who by that point knew me pretty well, came over and asked if I was Ok. I told her what had happened and she told me that I needed to stay positive and stay the course. She offered some counseling and said the hospital could make arrangements if I needed to speak to someone. Just the fact that she, and others noticed meant a great deal to me.
Later I wrote an email to the President and CEO of the hospital. I expressed my sentiments and the positive input I had around the cardiac rehab program in general and about the staff who had helped me so much in particular. I wanted these folks to get some recognition, and I knew from my previous work experience to start at the top. It’s much better when words of appreciation trickle down than if someone tries to push them up the corporate ladder. The CEO responded right away. She said she would send my email to the department heads and let them know and that eventually it would be communicated to the manager of the rehab center.
Based on the letter they asked if I could participate in a senior management meeting they had planned and to communicate my thoughts and field questions during this meeting. I told them I would be delighted.
The entire experience was another example of God’s grace helping me get through this tough time in my life. The people, the facilities, the medical system we have in this country are all part of God’s everlasting goodness. I had prayed so long for help during my years in heart failure. I had asked for the strength, and for healing but I had also acknowledged that his will be done. God provided all those people pulling me up the mountain and pushing me from behind and at the end of the day I felt like I had made it to the top.
The next post will be a breif review of the disease that was a the root cause of all of this. Cardiac Sarcoidosis.
© 2026 Phil Liaboe. All rights reserved.

Leave a comment