By Phil Liaboe
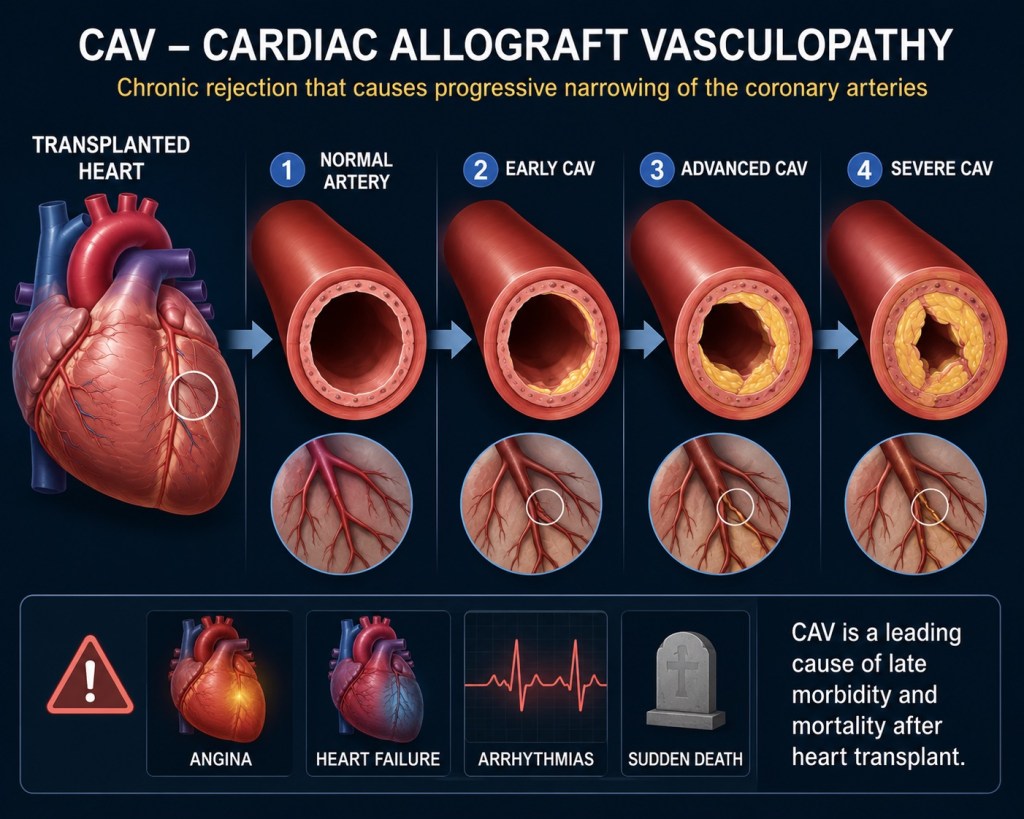
At about 1 year post-transplant I had a left heart catheterization (LHC). This procedure is routinely part of heart transplant protocol at my medical center. This is done mainly to check for CAV (Cardio Allograft Vasculopathy). For heart transplant patients CAV is known as the silent killer.
CAV is a chronic form of heart organ rejection characterized by progressive narrowing of the blood vessels in the graft (new heart). Because the heart is denervated, there are few warning signs or chest pains when it is occurring, hence the need for the left heart catheterization to check and determine if CAV is present.
LEFT HEART CATHETERIZATION
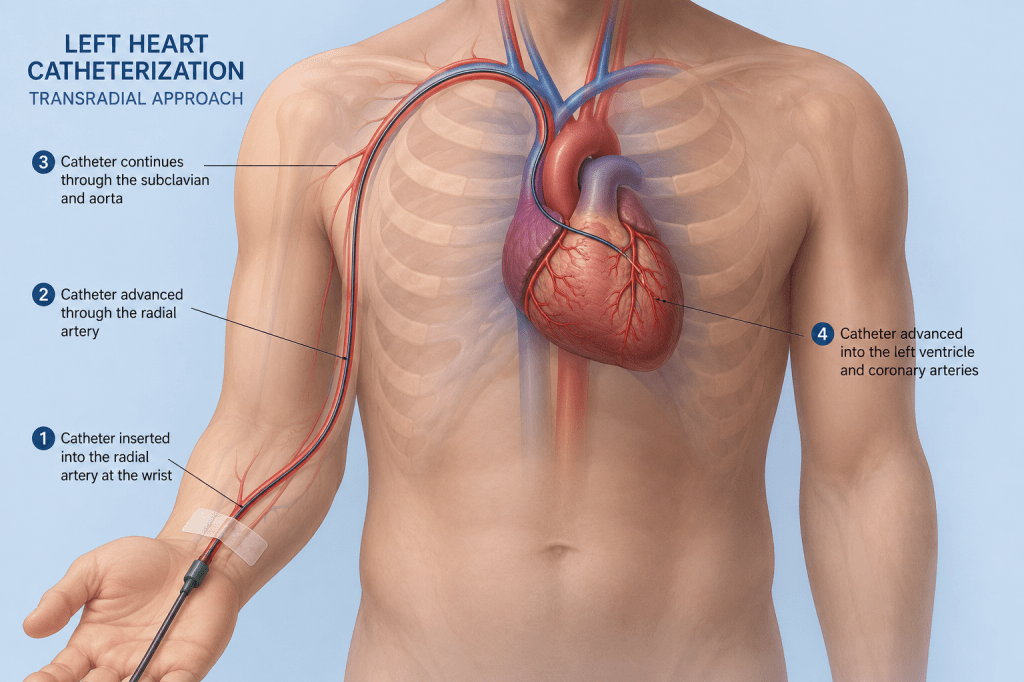
In a previous post I went into great detail on the Right Heart Catheterization (RHC). That was because heart transplant recipients have several (12+) after the operation to biopsy the heart and check for signs of organ rejection. The left heart catheterization is similar in concept; however, instruments are guided into the heart in a different way to check different aspects of heart function.
One difference between the LHC and the RHC for me is that in the catheterization lab during the procedure, the doctor entered the heart beginning in the wrist (artery) instead of the neck (vein). Also, for this I was mildly sedated. Afterwards, I woke up in the recovery area wearing a Terumo Radial Compression Device (TR Band)
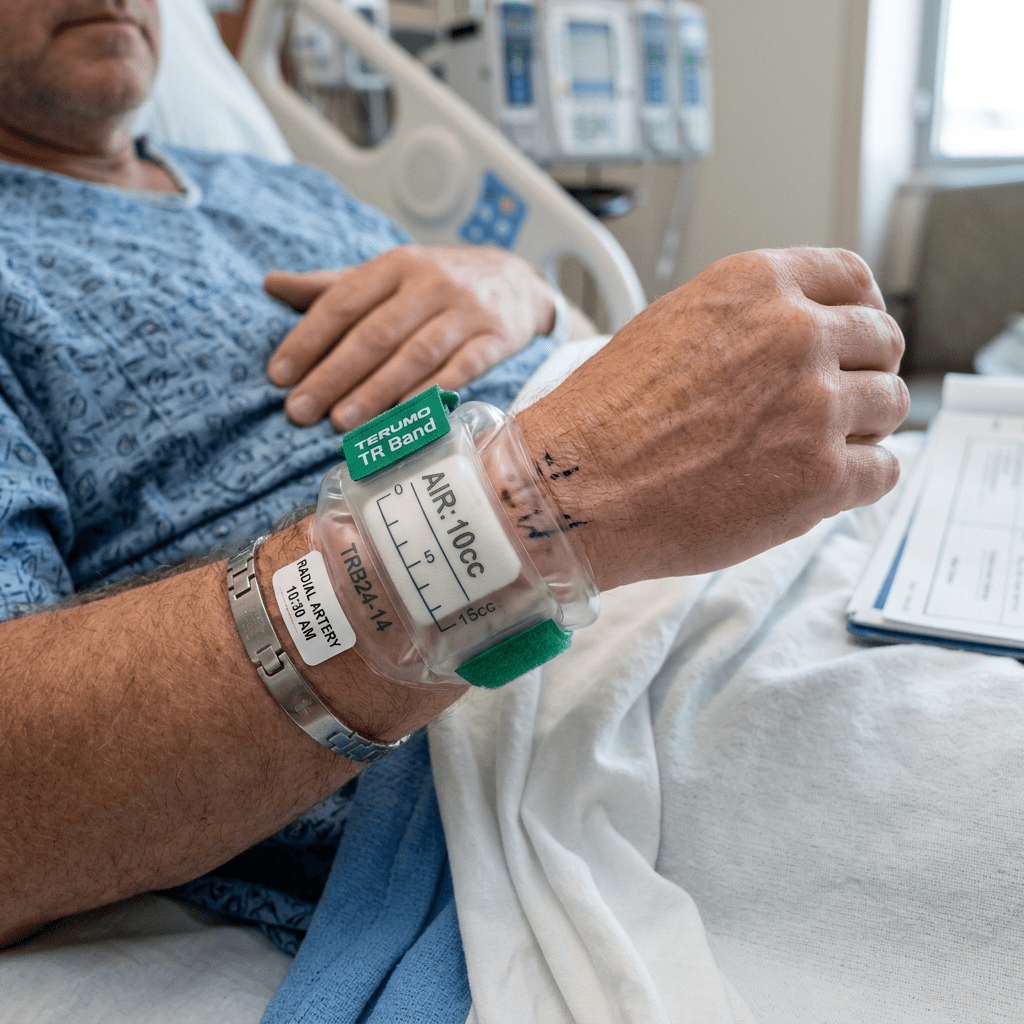
The TR band is inflated with air and that provides compression to prevent bleeding from the hole in the artery created during the procedure. I doubt this happens often but I had a mishap.
My wrist was resting by my side and I was using my other hand to scroll on my phone. Suddenly I felt wetness where my wrist was resting and I looked down to find my hand sitting in a shallow puddle of my blood. I panicked a little. I yelled “code blood!”. Not sure why I yelled that. I knew from TV shows various codes are used in hospitals when thing get urgent and I didn’t know what the code was for this so my Netflix soaked mind went to that phrase “code blood”.
It worked. This recovery area in this large medical center has patients lined up in spaces separated by curtains. Not sure how many spaces, but I would estimate that there are around 20. Given that, as you might expect, there are a lot of nurses and doctors coming and going. When I yelled for help, I had 5 people in my space in about 2 seconds. I was OK. They cleaned me up and pumped more air into the TR band for a tighter compression and extended my recovery time to be safe.
My LHC came back “moderate” for CAV. That is not the result anyone wanted to see, least of all me. CAV is not rare. A significant percentage of heart transplant patients have CAV but usually much later post-transplant. It is a disease process that cannot be reversed. With treatment it’s progression can be slowed or even stopped.
Time to regroup and reset again! A common treatment for CAV is to change one of the anti-rejection meds I was taking to one that has proven more effective at slowing or stopping CAV. Sirolimus {sear-o-lime-us} has shown to be more effective than one of the other anti-rejection meds I was taking called Mycophenolate {my-ko-fena-late}. Changing anti-rejection meds is tricky. To remove one and replace with another poses a risk of organ rejection.
Here is a summary of the steps:
STEP 1: Sirolimus is slowly brought into the daily medication regimen to therapeutic level, while Mycophenolate is slowly titrated out.
STEP 2: While this is happening the transplant team closely monitors if any signs of rejection are occurring through special blood testing at home (CareDx) explained earlier.
STEP 4: If the CareDx blood test shows signs of rejection then a heart biopsy / right heart catheterization is performed to confirm whether rejection is really happening.
STEP 5: (if needed) If it is, then the patient is admitted for three days of rejection treatment.
Yes, my Caredx blood work showed signs of rejection.
Yes, my right heart cath / heart biopsy was performed and confirmed I had organ rejection happening.
Yes, I was admitted for 3 days of organ rejection treatment.
Lauren and I saw the biopsy results on the patient portal and knew it was bad before the transplant team called. We were in the car coincidently going into Boston to meet family members for dinner when I got the call. I saw it was Beth Israel calling and I answered “Hello, this is Phil”. I heard a familiar voice on the phone say “Hi Phil, this is Amanda from Beth Israel”. I said “Hi Amanda, what room am I in?”. I knew before she called that I was going in. I am sure she was dreading breaking the news to me.
I hate to admit this, but Lauren recommended us packing a hospital admission gym bag and bringing it in the car just case while we met some family in the city. I said “Nah, they won’t call tonight”. Note to self: Listen to your spouse / caregiver.
Ok, so here I am, a guy who had cardiac sarcoidosis with advanced heart failure, a transplanted heart, recurring sarcoidosis, moderately deadly CAV and now organ rejection. Plus, I had neuropathy in my feet and kidney disease, both the result of reduced blood flow. I had a wrinkled macula that has made one eye almost blind (the cure is to stick a needle in there and peel off the wrinkled layer). I have the beginnings of osterperosis, the result bone denisty reduction from more than 6 years of daily prednisone. Oh, and hypothyroidism. I was gobbling a fist full of meds four times a day and topping that off with monthly infusions. I had reduced cognitive ability (according to my wife). I am on some kind of medical Tour de Force. A unicorn. Somebody will want to study my cadaver someday.
ORGAN REJECTION TREATMENT
The 3 days of treatment for organ rejection were easy. Each day I got a 3 hour infusion of steroidal medication. My treatment was a blast of 1,200 mg every day for 3 days or a total of about 3,600 mg. Other than those 3 hours I was free to do as I please, inside my hospital room.
Sleep was almost out of the question. This hospital stay was much different from the last one because I felt fine. Terrific even. Except for when I had the IV and a bag of fluid for a couple of hours, I was mobile. Frequent trips to the snack area to get hot tea and a bag of saltines. I hung out in my bed, on the lazy boy chair or on the mini sofa. I read a lot on my tablet and MacBook, annoyed the nurses, and walked around a little looking for anyone to talk to, not finding much. I am not a TV guy unless it’s a movie and the room had 20 channels, not all in English. Occasionally I would find a sports event but my interest in that has waned lately.
I tried doing some light exercise. Nothing crazy. Some chair squats, wall sits and planks. I had to wear the ever present heart monitor, so a nurse came in my room and saw me in a plank and asked what I was doing. I told her and she said to stop that. The displays were flashing an elevated heart rate.
I complained to my oldest daughter, who has three young energetic sons, about being stuck in my room. She said, “Dad! Wait! You sit in a room by yourself and you can do whatever you want all day? They bring you food when you want. It’s quiet all day long. And you are complaining?”
They were preparing my discharge on day three and noticed the iron level on my blood was low. They last thing they did before letting me go was an iron infusion. One for the road. Put it on the tab! I was told the side effect of getting a bag of iron infused was that I would feel like Superman. That did not happen. I just felt like me, which was mostly just grateful that the prognosis was good that this would halt the rejection.
WAIT AND SEE
It was a waiting game now to let my new treatments do their thing for a few months and see how it goes. My next test for rejection came back negative so that was good. I was starting the infusions to stamp out the recurring sarcoid and it would take 6 months or so to see if that was working. I was now taking Sirolumus to address the CAV and it would take several months to see results on that too.
I did have a 2 or 3 week period on the Sirolimus where I had visible red dots on my expansive forehead and sores and in my mouth. More good stuff! These side effects are normal. The red dots looked like pimples. The sores in my mouth were very similar to canker sores (aphthous ulcers). I estimate I had three of four under my tongue. I was prescribed a cream for those but I am not sure that did much good. The cream doesn’t stay in place. Eating anything stung for awhile. It was not a terrible hardship. All that went away.
After about 6 months I had another left catheterization to check the status of the CAV. That also came back as good news. It had not progressed which is about all you can hope for with CAV. It’s not reversible. The goal was to slow it or stop and on that test on that day it showed no difference from that last one.
That brings us up to the current status. I am so grateful for all the work done on my behalf. As I said in the introduction, the yellow brick road is winding and filled with scary surprises. Right now I am still recovering emotionally for all that took place. It was a double barrel hit that really left me very disappointed as I was emerging from the heart transplant. It was so much work, almost hourly constant vigilance for so long to yield these complications.
I had begun thought processes about what was next after transplant and I had taken some actions toward those ideas and then poof. Blown out of the water. It has made it difficult for me to think in terms of “what’s next” now. Maybe nothing. I feel like I have a lot to offer but not exactly sure what that looks like. It is hard for me to think and plan that way when I am in survival mode. It’s a work in progress.
There is a phrase that is asked of me at times that I don’t care for. People will ask “So, now that you have had the transplant, what are going to do?” The inference being that now I need to do something remarkable or substantial to justify having my life being saved. My combative nature, which I have tried hard to tame my whole life, wants to blurt out “Not sure. You have not had a transplant so what are YOU going to do?”. I stop myself though and just tell them I don’t know.
This brings me up the present day. One area I have not touched on is some of the events that took place before the transplant. For a couple of posts I will circle back to before the heart transplant and summarize experiences that occurred prior to the operation . Believe it or not there is much on this journey I have not disclosed.
One minute I was fine. The next minute I had heart failure.
© 2026 Phil Liaboe. All rights reserved.

Leave a comment