By Phil Liaboe
A Not so Slight Complication
My heart transplant had one unusual complication and it was very rare. Once a complication happens on this road there is a chain reaction. I can’t go into depth about how many transplant recoveries go without a hitch or how many have a lot of trouble. Most of the other people I have met or interacted with in the transplant support groups have had a pretty smooth ride. That is not a great way to sample for obvious and morbid reasons. It’s sufficient to say, as I did in the introduction, that each person’s journey is different.
Mine started off strong. I was home in 13 days. I was doing terrific through the early, 6 month high risk period and played 9 holes of golf at 4 months post-transplant. I was attending my cardiac rehab religiously. Actually, more than religiously because it was twice a week. I felt great. The shaky, wobbly feeling I had experienced early on, which was totally to be expected, was in the rearview mirror as I became more like myself both physically as well as mentally. My spirits were high. At times euphoric.
CRAZY RARE
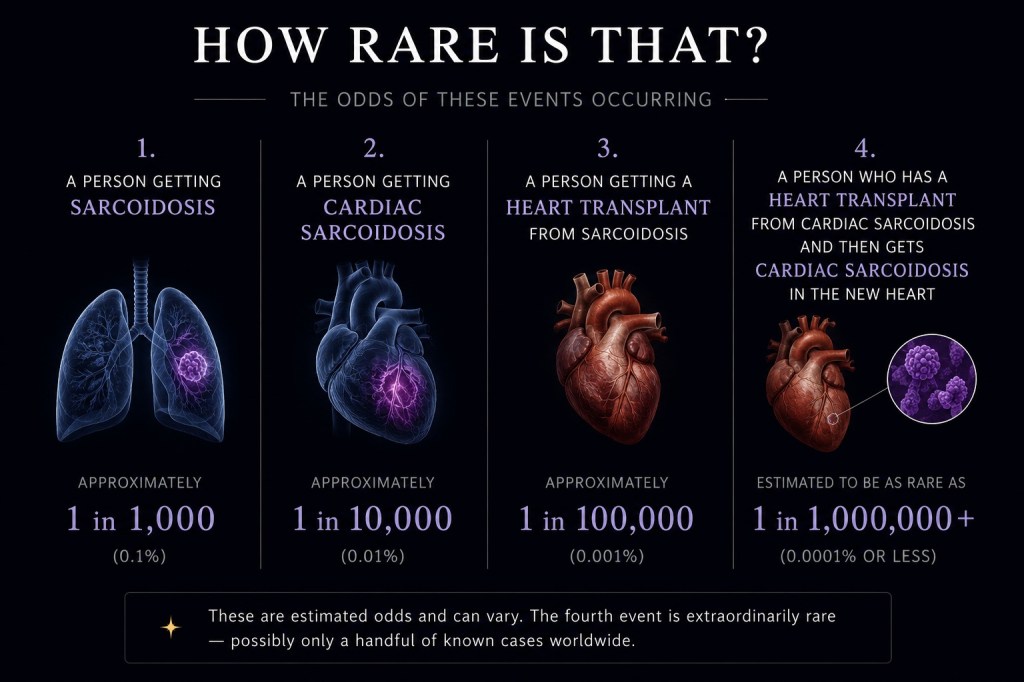
As was mentioned earlier in this writing the disease that claimed my native heart was cardiac sarcoidosis. It is a rare disease.
For those that like statistics it’s currently about 1 case per 10,000 people worldwide, which is less that 100th of 1 percent (.01%).
The number of cardiac sarcoidosis patients that result in a heart transplant is in the 1 – 5% range. So for every 1,000 cardiac sarcoidosis patients, a good estimate is that 10 – 50 will result in heart transplant.
Now to go even farther into the realm of the uncommon only about 10 percent of those patients who received a transplant due to cardiac sarcoidosis contract recurring sarcoidosis in the newly transplanted heart. In the general population that translates into 1 in 1,00,000+.
To put this into perspective, here are some events that also carry similar odds to recurring sarcoidosis in a transplanted heart:
- Being struck by lightning
- Winning a 5 number state lottery
- Being hit by a meteorite.
This is what happened to me. Cardiac Sarcoidosis reoccurred in my newly transplanted heart.
CARDIAC SARCOIDOSIS IN MY NEW HEART
Because of the fact that I had this rare disease initially, Beth Israel Deaconess thought it prudent to test for sarcoidosis post-transplant just to be sure it had not reoccurred. I am so grateful they did. It was a routine check.
To everyone’s shock and surprise, sarcoid had returned in my new heart. The gold standard for detecting sarcoid in the heart is the Cardiac PET scan. I had my first post-transplant PET scan 6 months after the transplant. After that first PET scan my coordinator on the transplant team reached out to me to ask me if I had followed the pre-scan recommended diet correctly. I emphatically swore that I had. To the letter. It’s a strange diet and Lauren and I had made sure that I complied. This was not our first cardiac PET scan prep.
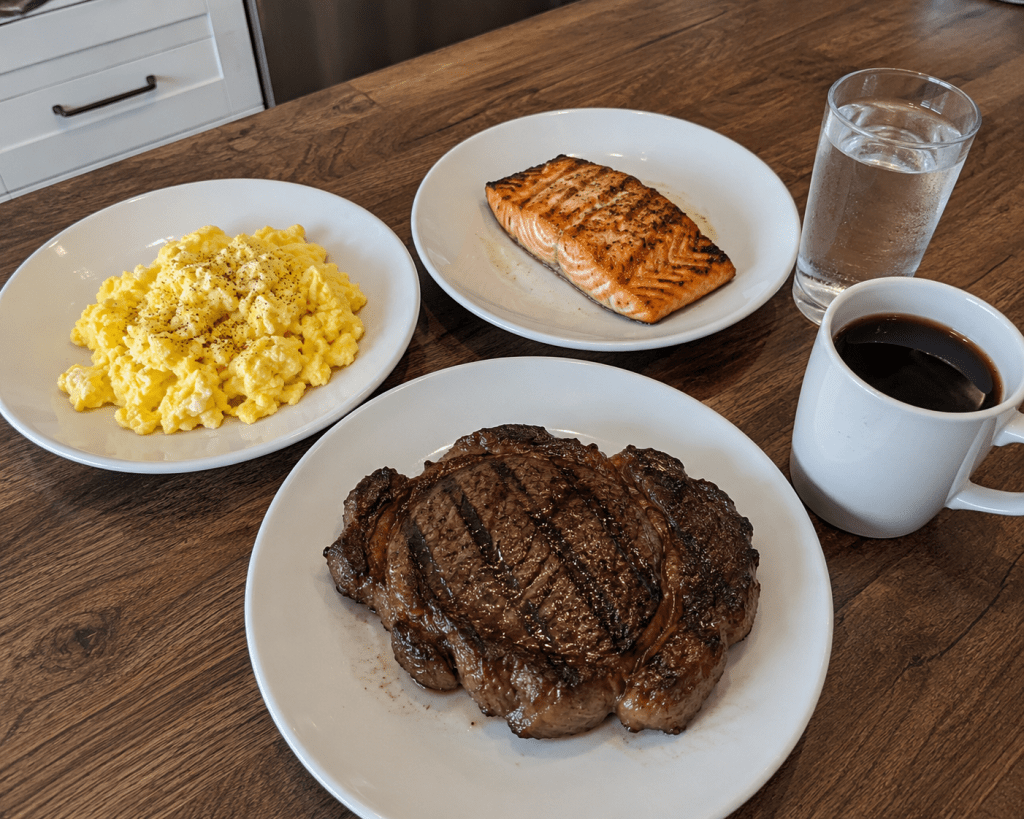
(typical Cardiac PET Scan diet)
After those first Cardiac PET Scan results came back, my coordinator said some of the imaging was unreadable and they wanted to repeat the test only this time I had to follow the unusual diet for two days not one. This diet is basically a diet of fatty meat, or eggs, and nothing else but the butter you cook it in. So 2 days of eggs (only) in the morning, salmon or a hamburger patty at lunch and a rib-eye steak for dinner. That is it! Nothing else except salt and pepper and black coffee or water. We repeated the test after the strict two day diet.
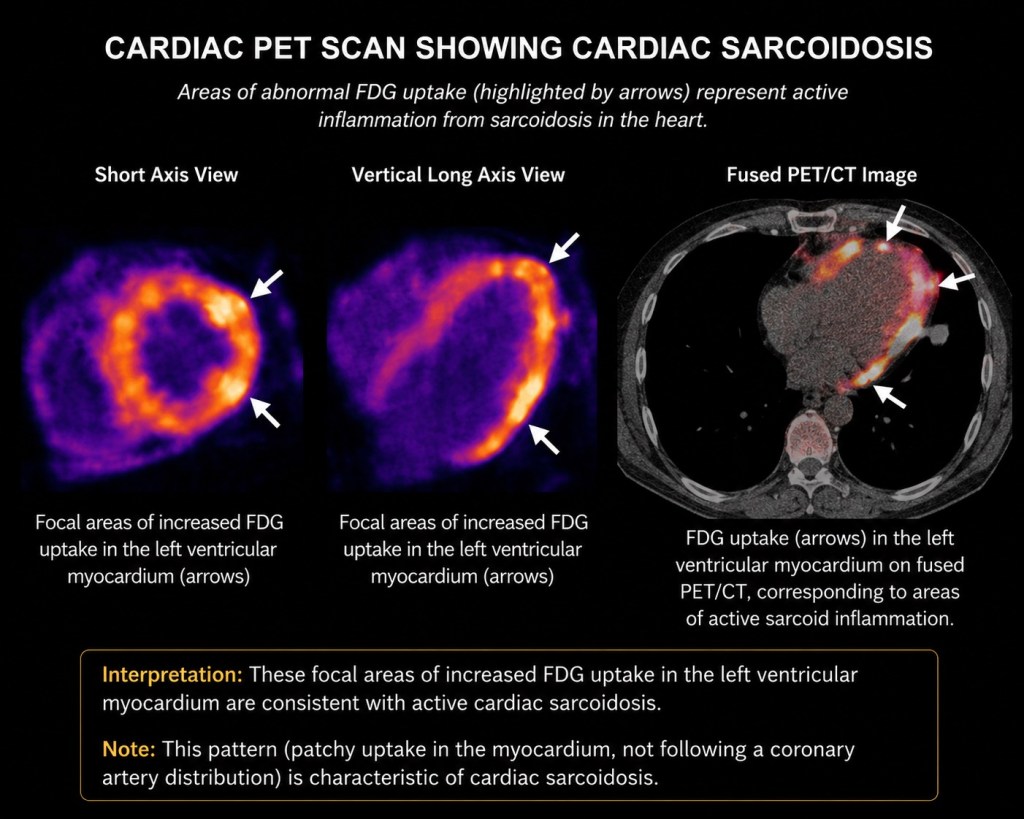
After the 2nd PET scan the transplant team dropped the bomb on us that sarcoidosis had returned in my new heart. In the image above, FDG uptake refers to the contrast that is showing where the sarcoid is present. Nothing else but sarcoid takes on this appearance in a Cardiac PET scan. They told me they saw it on the first PET scan but questioned the results. They did not want to alarm me in the event there was in fact an error of some kind made on the first test. After this second test however, there was no doubt. For me this was an emotional sucker punch combined with a kick in the teeth.
It’s easy to read something like this and think, wow that’s bad, and kind of move on. The emotions are hard to describe considering all that had transpired for me to that point.
- More than 3 years of advanced heart failure.
- Over a thousand nights trying to get to sleep thinking the chances are even that it was the last time.
- The trauma of the transplant both physically and emotionally.
- All that I had dragged Lauren and my family through along with my extended loved ones.
- Diligently following each and every weekly, daily and sometimes hourly directive as closely as I possible could after the operation.
- Countless heart biopsies, chest x-rays, cardiac echo’s, MRIs, and weekly blood draws. I had done my very best in every regard.
- All to get right back where I started from with a disease that had wrecked my first heart, and had no known cause and no known cure.
It was a crushing blow. I hated telling my family and spreading the sadness. One of my daughters said she was pissed off.
Remember when I said to get on the transplant list a patient has to prove that they are a good risk because nobody wants to waste a donor heart? Well, nobody at Beth Israel Deaconess has told me this but you don’t have to be a rocket scientist to guess that I would likely no longer be able to qualify for a re-transplant. Quite simply I would not be a good risk. What was running through my mind was that now I have to try to survive as long as possible with recurring cardiac sarcoidosis. What would that look like? Not pretty.
RESET
Once the dust settled for everyone we had some meetings with the specialists on my cardiology team and re-grouped for the new plan. Sarcoid had wrecked my old heart, true. But nobody knew how long it was present before I nearly keeled over raking wet leaves in the fall of 2018. How long did I have this thing before I started showing symptoms? Unknown. Monthly infusions of Remicade (aka Infliximab, Inflectra etc.) had stomped it out. Scarring was left behind that rendered my old heart severely weakened.
Now we knew that sarcoid had only been in my new heart a relatively short period of time and the PET scan showed signs of sarcoid, but it was not rampant (my medical term). The thinking now was to have me go back on monthly Remicade infusions ASAP to stop the spread. A great metaphor they used was a burning house. With my first heart the fire could have been, and likely was, burning for a long time before any action was taken. Once that fire was put out what was left behind was still standing, but not much use. This time with my transplantedd heart, the house fire had just begun. Maybe it had not even turned into a real fire yet. Perhaps it was just smoldering. Get back on the infusions. Put out the fire before it can do any real damage. So, this what we did.
Oh, my doctors said, and by the way, now that we know that you have cardiac sarcoidosis again, and we know the first time it made you susceptible to ventricular tachycardia, we highly recommend you get a defibrillator re-implanted. The hits just keep on coming. Ouch! This was not a mandate. My doctor handling the electrophysiology (EP), who by the way is world renown, told me it would be a good idea.
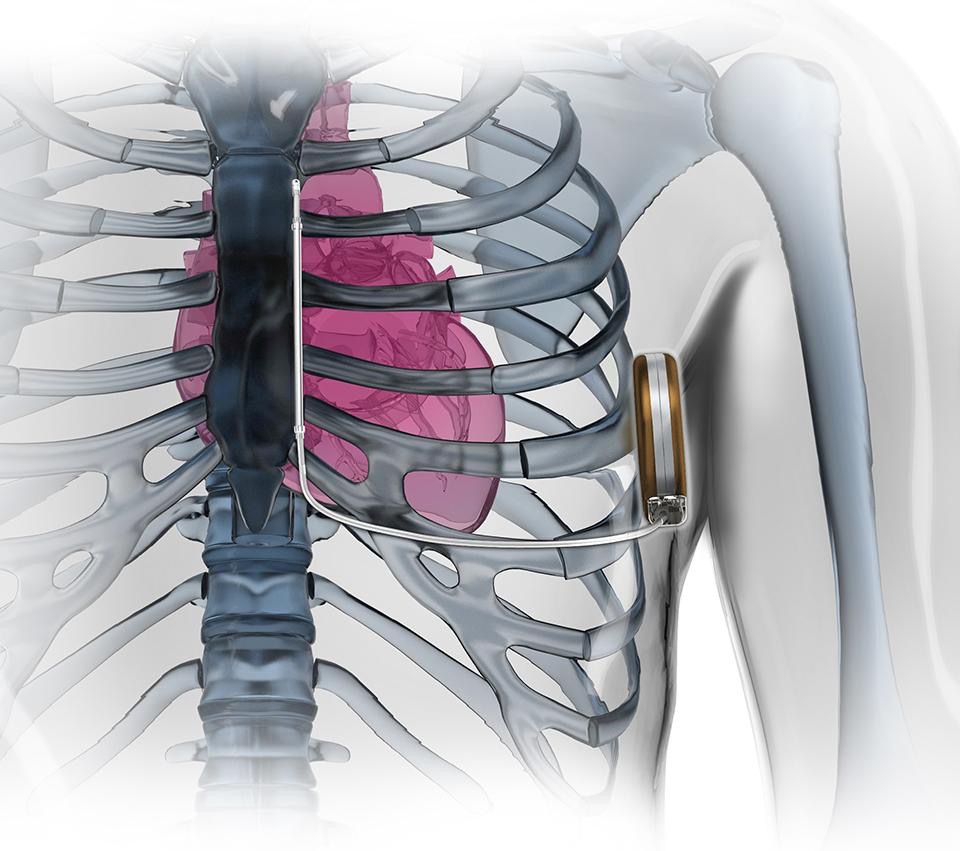
I will tell you right now this was a little painful. The incision made by this surgery was kinda angry afterward for awhile. Perhaps it is just a sensitive area. It burned for several days. I was checking my watch for the next round of Tylenol for a week. Instead of my previous multipurpose ICD implanted just under my left clavicle, this one was implanted 6 inches under my left armpit, on my side. See above image.
To say its size is in the neighborhood of a can of tuna is not an exaggeration. This defibrillator is not connected directly to the heart. It is connected to a sensor about the length of a pencil (but thinner) that is also implanted on top of the sternum. The lead that connects the device to the sensor snakes under the rib cage. Because it is not coupled directly to the heart, but rather resides on the chest, the amount of energy it provides during a defibrillation event is much greater than my old one. So, I asked, that means a bigger shock? They said yes. Terrific!

And just like my old ICD, this one has a bedside monitor. I a press the button once per week to send a transmission showing my heart activity back to the EP team at the medical center.
Side note here on that bedside monitor: After a couple of months the EP folks called me and asked if I could come in soon. They saw some “static” in the readings. Keep in mind they are talking about my heart. I told them I was due into Beth Israel for a normally scheduled clinic meeting the following week and could I do it then? They said they want me to come in today, or tomorrow at the latest.
We went in that day. Well, it turns out I am left-handed and moving my arm quickly back and forth, rubbing against the defibrillator was causing some unusual readings. It’s not what you think. See, I have this hobby selling used golf balls. I sell about 30,000 – 40,000 golf balls a year as a fun side hustle and I clean them all. You read that correctly. I wrote a book about it. That rubbing motion was causing what they called static. They tweaked the tolerances or something (I have no idea) in the way the sensor works that removed the static and sent us home. Every day is an adventure on this ride.

So I hopped back on the monthly infusion train. As of this writing I have been having monthly infusions of Infliximab for about a year. I have had 2 Cardiac PET Scans to see if it’s putting out the fire (reducing the sarcoid in my heart). On the most recent PET scan, the tech doing the scan recognized me. He wanted to know why I was back so soon. I told him about the recurring cardiac sarcoidosis. He said, “Wow! Dude, that sucks!.”
I am pleased to report that so far it appears to be working. The comparisons from one test to another show that the prevalence of sarcoid has been reduced. Not gone yet. Hopefully that will be shown on the results of my next PET Scan about 2 months from now. And, thankfully, heart function is good. No VTACH. No shocks. No new scaring. Last week I achieved a personal goal of walking 18 holes of golf. I started a Facebook support group for people who have had recurring cardiac sarcoidosis in a transplanted heart. So far I have one member. Me.
This was not the only problem I encountered around the same time frame. Just as I was reeling on the news of recurring sarcoid, I was introduced to a new challenge called CAV, which stands for Cardiac Allograft Vasculopathy. Hint: It’s not good.
© 2026 Phil Liaboe. All rights reserved.

Leave a comment