By Phil Liaboe

The acronym ICD stands for Implanted Cardiac Device. The term ICD encompasses a broad range of cardiac devices including pacemakers, defibrillators, and other cardiac assist implants. Some devices perform several of these functions all in one unit. The ICD device I had implanted early in my advanced heart failure diagnosis was a CRTD, or Cardiac Resynchronization Therapy Defibrillator.
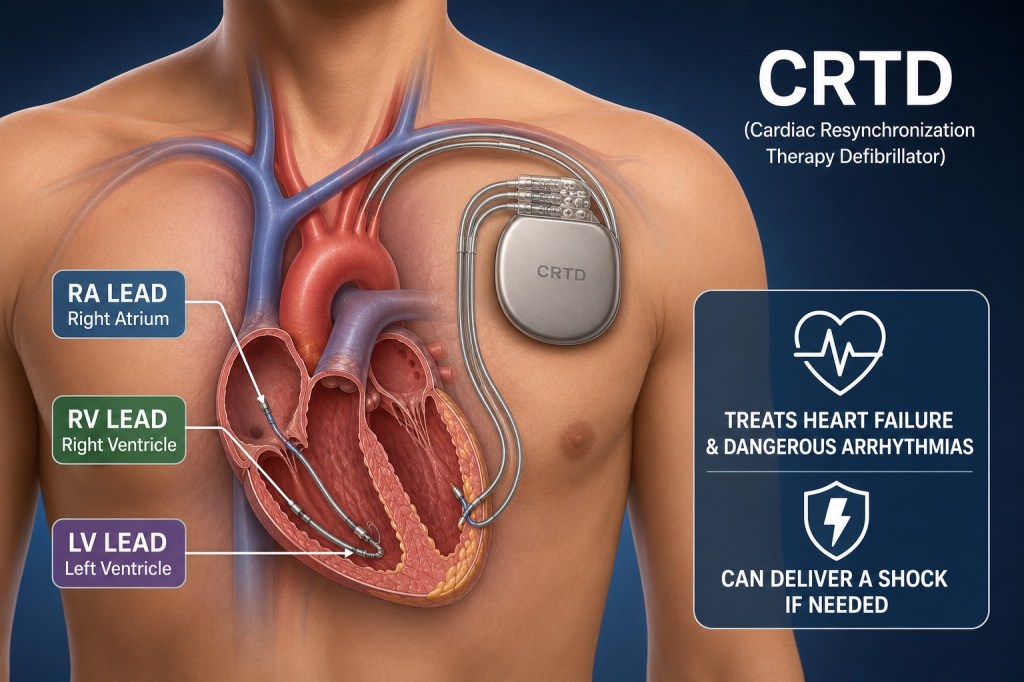
One way to explain what a CRTD does is to break down each of its 4 major functions. They are as follows:
- Pacemaker: This function sends tiny electrical signals to the heart to achieve a steady heart rhythm. At the time mine was implanted my heart rhythm was very abnormal and I needed the pacemaker function to keep me in a normal heartbeat. Some other patients I have spoken to have said they could feel when the pacemaker tripped on or off. I never felt anything. That was likely because it was pacing, or engaged, almost all the time.
- Resynchronization: The resynchronization function provides help to the heart to keep all of numerous heart actions firing off in the right order and the right time. I never had an awareness of this function. I could not feel the device engaging. It was doing its job in the background.
- Defibrillator: This is exactly what sounds like. It is not my intention to frighten or worry anyone who might have one or is considering an implanted defibrillator as I later describe what is it like when it is called into action. It’s a lifesaver. The device has settings that are customized for each patient. The defibrillator will engage if one of those settings is breeched. For me, I had an upper limit of 220 beats per minute (BPM). There is also a setting at the low-end and I think mine was 40. My heart disease caused Ventricular Tachycardia. This is very rapid heartbeat where they heart is pumping so fast the chambers don’t have time to fill up. If my heart rate exceeded 220 BPM, the defibrillator would deliver therapy to bring me back to sinus rhythm. The therapy delivered is an electrical shock. The amount of energy my CTRD delivered was 41 joules. That is a fairly small amount of electricity. It’s about what is needed to power a 100 watt light bulb for .4 seconds. What makes it effective is the energy is delivered in a very short burst. Bang! It’s hits hard and then it’s gone. People have asked me if it hurts. It does, but only for a split second. The analogy I’ve used is to imagine getting hit by a major league baseball pitcher with a fastball square to the sternum. But no pain afterward. Just the memory of it. It happened to me six times over a period of 2 years.
- Monitor / Data Collection: A sometimes overlooked function of this kind of device is it’s capability to collect and transfer data. With mine, I had a bedside controller that with the weekly press of a button, enabled a data relay back to the medical center for review. In addition, on a quarterly basis I would visit the Electrophysiology (EP) Department and the implanted device would undergo a deeper data integration. The term interrogation is used by the EP folks and it simply means that as a patient I would sit in a chair while a round device called a Programming Wand is rested over the CRTD on my chest and a higher level of data is transferred that way as well.

The Programming Wand is connected to a briefcase size piece of equipment called the Programmer. The Programmer allows the EP nurse to do the following:
· Provide remaining battery life in the CRTD
· Lead impedances and performance
· Pacing percentages
· Recorded arrhythmias
· Device settings and therapies
The responsibility for the recommendation, implant and on-going follow-up rests squarely on the in Electrophysiology (EP) department the medical center. EP is a specialization of cardiology and is concerned with the electrical signals that control heart function. For all intents and purposes, the implanted CRTD is permanent, with one exception. It will be removed in the event of a heart transplant, as mine was.
The device is approximately the size an old-fashioned flip phone or if you are as old as I am, a handheld stopwatch. It could fit in your palm. For me, it was implanted in the left side of my upper chest, just below the collar bone, more toward the shoulder than the chest center.
Metal wires called “leads” run from the device to the heart. These leads are attached to the heart. Logically one does not want one of these leads to ever come loose or detach from the heart. Therefore, the leads are affixed to the heart with tiny threaded screws. I was told that once they are attached, it’s very hard to get them out. By design.
MY PERSONAL EXPERIENCES
In all that has happened to me in this whole heart failure and transplant journey, the only time I had what could be called a panic attack was walking into the operating room to have my CRTD implanted. Before the operation I was briefed about the risks and the anesthesia and signed the forms that indicated that I understood. Standing in nothing but my johnnie, they pointed to the O. R. double door. I went in. I saw a large room with enormous monitors and in the middle was a table. People were busy getting ready. They were dressed like surgeons. Whoa!
That was when it hit me like a 2 by 4 across the head. I was supposed to lay down on that table and they were going to cut into me and attach this device to my heart. My instinct was to run. I almost did. It took everything I had not to. It would have been quite a scene. Tufts Medical is right next to Chinatown in Boston. I could almost see my bare ass hanging out the back of my flapping johnnie while sprinting down Tremont Street with orderlies chasing me. I pulled it together and reclined, down on the table.
While I was in recovery I was joined by two of the EP doctors checking on me. Lauren was there as well. She had seen a movie recently where an assassin had eliminated his intended target by hacking his pacemaker. So Lauren asked if my device could be hacked. The room went silent for a few beats as everyone let that question sink in. The two doctors were looking at their clip boards and at each other out of the corners of their eyes, hoping the other one would answer. Turns out it can be hacked, but its extremely hard to do. Good to know!
I will not go into the history of the development of these devices. There is a rich and amazing background story for how these lifesaving devices were invented and how they have progressed. Here are a few of the most notable attributes that I think folks would be most interested in and how they affected me.
Device Set-Up: Shortly after the surgical implant the EP nurse came in into my hospital room with the Programmer and Programmer wand. She said she needed to set it up with custom settings. This was a crazy experience. First, using the Programmer device and Wand she tested it by increasing and decreasing my heart rate. Imagine lying in a hospital bed and a nurse touching a screen that makes your heart start beating faster. Noticeably faster. Very strange.
It took some doing to get everything working properly. The medical center even needed to bring in the factory specialist (Boston Scientific) to vector in the right coordinates. I had a problem where my diaphragm was being stimulated by the device and they struggled to stop it. It was like a mega hiccup. It would occur randomly. My whole body would flinch. In this entire heart failure transplant journey this may be the weirdest thing I ever felt. They figured it out, eventually.
Heart Pacing: The download data will tell how reliant you are on the pacing feature. For example, I was being paced at 96%. The pacemaker was initiating or controlling 96% of my heart beats and my heart was contributing 4%. I know people who say they could occasionally feel the pacing. I never did.
Measuring PVCs (Premature Ventricular Contractions): The CRTD collects data at the same it is performing its intended functions. During the device interrogation described earlier it provided detailed data to the doctors about my PVCs. I was having a lot of PVCs. These feel similar to a palpitation or skipped heartbeat. On one download I was told that during the previous 3 months I had experienced 1.2 million PVCs. I felt them almost continuously for 3 years.
Battery Life: The device is battery powered. I was told the battery life was about 10 years. My assumption is that battery life will change rapidly with technology and only get longer. If the battery begins to show that it will run out, the device, often referred to as the “can” is replaced. Not the leads, just the “can”. Yes, that would entail another surgery.
Defibrillation: One of the world’s greatest examples of using a euphemism is referring to a defibrillation event as “delivering therapy”. Nobody wants to call it what it is, which is an instantly and brightly painful electric shock. It is a hard “thump”. I won’t explain the circumstances behind each of the six therapy delivery events I had. In one of the early James Bond movies entitled “Diamonds are Forever”, Bond (Sean Connery) gets roundly beat up by two women named Bambi and Thumper. YouTube the 3 minute clip and watch it. I named my CRTD “Thumper”.
It might help to know that I did quickly figure out when a shock was coming. My VT would start to become apparent when I would begin to feel what I can only describe as “ill”. Kind of sick. Then I would check my heart rate on my Apple Watch and see that it was increasing in speed like a runaway train. If my heart rate would get to about 150ish it would take off and not stop rising until I got shocked. That sick feeling would at least give me some warning to sit down or get ready. I could swear that just prior to the shock I could hear or sense a very slight high-pitched buzz, as if the device had been triggered and was spinning up to let loose the charge.
I quickly developed a mild PTSD behavior of obsessively checking my heart rate when doing almost anything that would cause a heart rate increase. If I hit 140 BPM, I would stop whatever I was doing and sit down hoping it would come back down on its own. I was taught by my medical team to “bear down” when my rate began to rise. Bearing down means clenching or tightening the abs and torso like straining to have a bowel movement. Another way to describe it is to try exhaling while blocking your exhale passages.
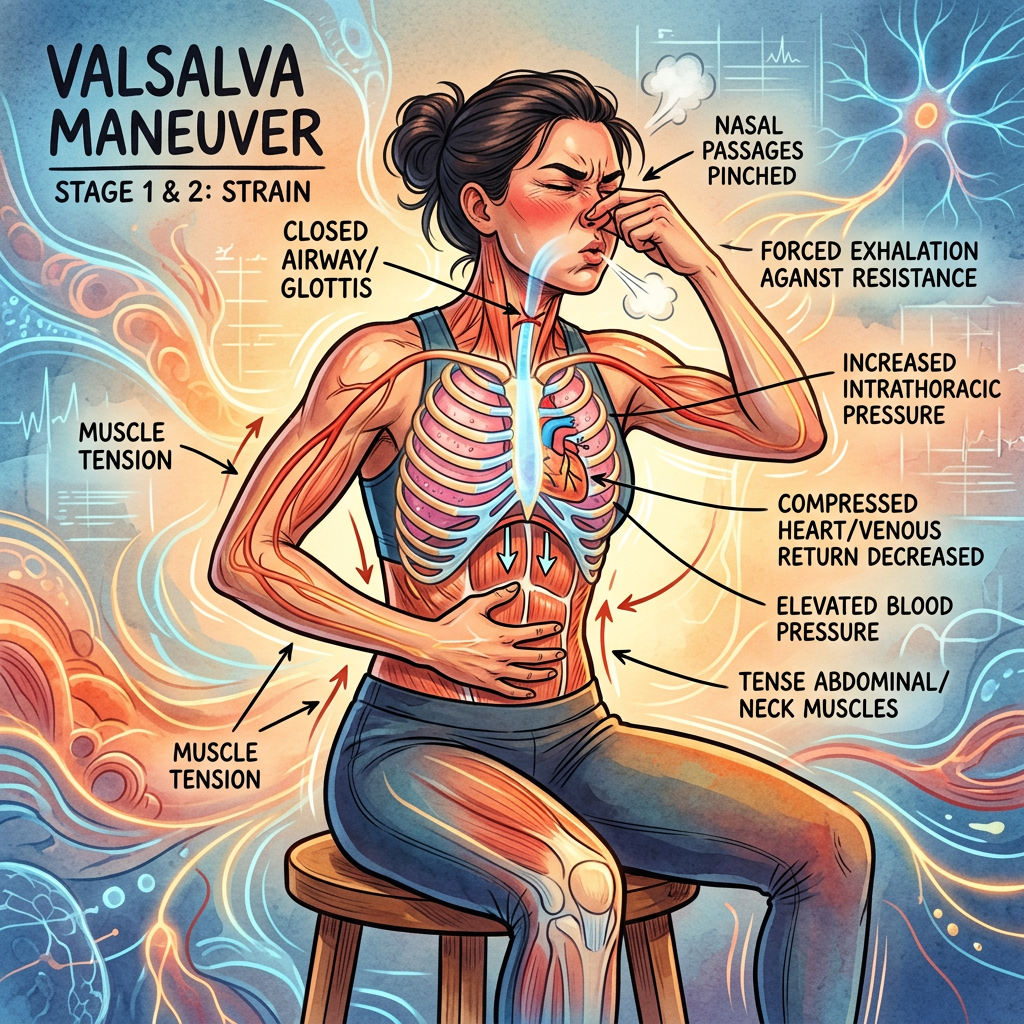
In medical terms it’s called the Valsalva maneuver. This action increases the pressure inside the chest and compresses the veins which reduces blood return. With less blood filling the heart, less blood gets pumped out. The body senses this change and drops the heart rate to compensate. It’s a temporary fix. It works. I did this several times and it helped interrupt the heart rate climb that was occurring.
The first time I was zapped I had no idea what had happened. I was playing golf. I had found my tee shot in a patch of rough grass that was between two fairways. The fairway I was on was playing in one direction, the adjacent fairway was playing in the opposite direction, and my ball was resting in some high grass in between. I could see a group playing on the adjacent fairway and I was wary they might be hitting in my direction. Out of nowhere my defibrillator fired off. Wham!
My first thought was that the group of players in the adjacent fairway had hit a strong line drive right into my chest and had not yelled “fore”, as is the golf etiquette. I screamed and grabbed my chest. I looked around. I slowly realized what had happened. It did not knock me down. The pain was instantaneous and tremendous. Then it was gone. I felt better. I was wondering if I should keep playing but the wise and close friend I was playing with advised we better stop.
It happened once it the shower. From that point on, I showered, shampooed, soaped down, and dried off just as fast as I could. After doing all that at top speed you won’t be surprised to know that my was heart rate was up!
The last shock I got I felt coming a mile away and tried to lay down on my bed with Lauren holding my hand. I was praying for God to help me when the shock came. On this one I felt like one of those Road Runner cartoons where once again Road Runner gets the best of his nemesis with an electrocution. Wylie E Coyote’s limbs, hair and eye balls all shooting straight out. I swear I saw lightning bolts in both my eyes when this one hit me. My wife had called 911 and by the time they arrived I felt fine. I always felt fine after the shock. Good even. The CRTD did it’s job wonderfully by forcing my heart back into sinus rhythm. The EMTs took me into the medical center anyway.
Once you are shocked by an implanted defibrillator the Commonwealth of Massachusetts suspends your right to drive a car for 6 months minimum. With good reason. If someone were to be shocked behind the wheel it could mean a tragic situation for the driver, any passengers, and any other vehicles or pedestrians on the road. Every time a shock is administered, the 6 month clock starts over. I lost my right to drive for over 2 years. I have conversed with others who had ICDs that had shocked them and they claimed they paid no attention to this driving rule and drove anyway. Sometimes I wonder if there are any bounds to human selfishness.
I could sum up my first year and a half of being in advanced heart failure as being fairly unstable. My implanted CRTD had shocked me out of dangerous VT heart rhythms 6 times in that period. I was starting to get a little obsessed about my heart rate because I knew if it climbed above 140 or 150 walking up a slight incline that it was likely to take off and climb to 220 where the CRTD was set to “deliver therapy”. I was shocked twice on the golf course, once in the shower and once just doing nothing but reading the mail.
On the last shock I had been admitted to Tufts Medical Center for the 4th time in a little more than 2 years. All these shocks are really not very good for the heart. Clearly it is better than the alternative. The next step suggested my the Cardiology team at Tufts was to have a cardiac ablation. The main goal was to try to stabilize my heart and stop the defibs. So that’s what we did.
In the next post I will describe what a cardiac ablation was like for me.
© 2026 Phil Liaboe. All rights reserved.

Leave a comment